
Abstract
Post-Stroke Bipolar Affective Disorder in the Elderly: A Case Report and Literature Review. Suteevan Cholitkul, MD; Suwitda Cholitkul, MD; Kamal Masaki, MD (Advisor); Samuel Gadam, MD; Warren F. Wong, MD.

Abstract
E N D
Presentation Transcript
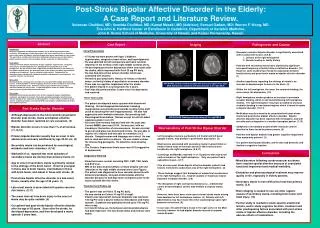
Post-Stroke Bipolar Affective Disorder in the Elderly: A Case Report and Literature Review. Suteevan Cholitkul, MD; Suwitda Cholitkul, MD; Kamal Masaki, MD (Advisor); Samuel Gadam, MD; Warren F. Wong, MD. The John A. Hartford Center of Excellence in Geriatrics, Department of Geriatric Medicine, John A. Burns School of Medicine, University of Hawaii; and Kaiser Permanente, Hawaii. Abstract Case Report Imaging Pathogenesis and Course METHODS Introduction Numerous emotional and behavioral disorders occur following cerebrovascular accidents. Although post-stroke depression is the most common of these disorders, post-stroke mania and bipolar affective disorder have been reported on rare occasions. The psychiatric and behavioral disorders following cerebrovascular accident reduce patient autonomy and increase caregiver burden, especially in elderly patients. Case report A 76-year-old male patient with history of type 2 diabetes, hypertension, congestive heart failure, and hyperlipidemia was admitted to the hospital because of left hemiparesis. He was found to have a right-sided cerebral infarction in the territory of the middle cerebral artery. He developed post-stroke depression which improved with antidepressant treatment. He also had post-stroke seizure. Subsequently, he developed manic episode with combative behavior and abnormal sexual behavior. His cognitive function also declined. Discussion Neuropsychiatric consequences of stroke are associated with multiple predisposing factors. Left frontal lobe or left basal ganglia lesions have been found to be associated with post-stroke depression. Anatomic lesions in post-stroke mania or bipolar affective disorder are not as clear. A right hemispheric lesion in a limbic connection area may be associated with post-stroke mania. Conclusion Emotional and behavioral disorders after strokes negatively impact rehabilitation, cognition, and long-term recovery. Evaluation and pharmacological treatment may improve quality of life, especially in elderly patients. Further study is needed to locate specific anatomical lesions associated with these psychiatric and behavioral disorders and cognitive function. • Initial Presentation • A 76 year-old male patient with type 2 diabetes, hypertension, congestive heart failure, and hyperlipidemia. • He was admitted for left hemiparesis and had a cerebral infarction in the territory of the right middle cerebral artery. • He developed post-stroke depression within one month after the stroke, which improved with Paxil 20 mg PO daily. • He also had post-stroke seizure disorder which was controlled with Dilantin. • He had no past psychiatric history, no history of alcohol abuse, no family history of psychiatric or memory disorder. • There was no cognitive impairment after the stroke. • The patient stayed in a nursing home for 3 years. • Paxil was discontinued after 2 years since his depression had resolved. • Three Years Later • The patient developed a manic episode with disordered thinking. He had inappropriate behavior including inappropriate sexual behaviors towards nursing home staff (such as touching the staff inappropriately). He also had aggressive and combative behavior, like punching staff. • Neurological Examination: Normal except for old left-sided • weakness grade 4 out of 5. • His short-term memory had declined over the past year. Current MMSE score was 20/30. He was alert, with no clouding or fluctuation of consciousness. He was oriented to person and place but disoriented to time. He was able to register all 3 objects and was able to remember 2 of 3 objects. Comprehension and language were intact. He was able to read and write a sentence. He was unable to draw the intersecting pentagons. He failed the clock drawing task. • The Geriatric Depression Scale score was 9/15 (suggestive of depression). • Diagnostic Work-Up • Blood tests were normal, including CBC, CMP, TSH, folate and B12 level. • MRI of the brain showed diffuse cerebral atrophy with old infarction of the right middle cerebral artery (see Figure). • The patient was diagnosed to have vascular dementia with • behavioral problems, and post-stroke bipolar affective • disorder because he had depressive symptoms prior to the manic episode after the stroke. • Treatment and Follow-Up • The patient was on Plavix 75 mg PO daily. • He was started on Celexa 10 mg PO at night. • Dilantin was tapered off, because Depakote was started at 125 mg PO twice a day for behavior disturbance and manic episode. Depakote was gradually titrated up to 750 mg PO twice a day. • At 3 month follow-up, the behavior and mood disturbance had both improved. His functional status and memory were stable. • Secondary mania or bipolar disorder is significantly associated with 2 concurrent factors: (2,5,8) • 1. Lesions of the right hemisphere • 2. Genetic loading or family history • Patients with secondary mania had a statistically significant increased frequency of family history of affective disorder. (10) However, some studies have found no association between family history and post-stroke mania or bipolar affective disorder. (1) • Another hypothesis regarding the etiology of mania is an increase in dopaminergic turnover in the brain. (5) • Within the left hemisphere, the lower the serotonin binding, the more severe the depression. (10) • Right hemisphere strokes produce an increase in serotonin receptor binding, which is not found following left hemisphere strokes. The right hemisphere may have an ability to increase serotonin binding in non-injured regions which is found in mania or bipolar disorder. (10,14) • Medication was also found to be associated with post-stroke mania and post-stroke bipolar affective disorder. Bipolar affective disorder has been reported with mirtazapine, and with steroids and cyclosporine in a cardiac transplant patient. (7,12). • Symptoms of secondary or post-stroke mania are almost identical to those found in primary mania. (5) • Patients with bipolar disorder had greater cognitive impairment than mania-only patients. (3) • Our patient had bipolar disorder, and he also had dementia and decline in cognitive function. MRI BRAIN: Diffuse cerebral atrophy with increased signal in the right MCA distribution consistent with old infarction of the right MCA Post-Stroke Bipolar Disorder • Although depression is the most common psychiatric • disorder post-stroke, mania and bipolar affective • disorder have been reported on rare occasions. (2) • Bipolar disorder occurs in less than 1% of all strokes. (11,13,15) • Primary bipolar disorder usually has an onset in late adolescence and early adulthood, by age 20-30 yrs. (5) • Secondary mania can be produced by neurological, • metabolic and toxic disorders. (4,16) • Starkstein et al. reported that most episodes of secondary mania are shorter than primary mania. (3) • Age of onset of secondary mania is primarily related to the etiology of the brain lesion. Onset is youngest in those due to brain trauma, intermediate in those with brain tumor, and oldest in those with stroke. (5) • Post-stroke bipolar affective disorder is a late-onset • illness, usually after the age of 40 years. (1) • Late-onset mania is associated with greater vascular risk factors. (3,11) • The mean interval from brain injury to the onset of • mania may be quite variable. (5) • Our patient had post-stroke bipolar affective disorder after the age of 65 years. Soon after the stroke, he developed depression, and then developed a manic episode 3 years later. MRA BRAIN: Bowing and narrowing of the right MCA Neuroanatomy of Post-Stroke Bipolar Disorder • Left hemisphere lesions, particularly left frontal and left basal • ganglia lesions, may produce a post-stroke depression. (3) • Most lesions associated with secondary mania involved limbic or • limbic-related areas of the brain and all of these lesions were • localized to the right hemisphere. (5,9,11) • Cummings and Mendez reported 11 of 12 patients with mania had • cortical lesions of the right hemisphere. Only one patient had a • subcortical lesion. (3,17) • Five of seven post-stroke bipolar affective disorder patients had • lesions restricted to subcortical area of the right hemisphere. (3) • These findings suggest that disruption of subcortical mechanisms in the right hemisphere (i.e., head of caudate or thalamus) may be important in bipolar disorder. (3,8) • The disruption of right cortical mechanisms (i.e., orbitofrontal • cortex or basotemporal cortex) may mediate a unipolar mania. • (3,8) • However, there have been a few cases of post-stroke mania arising from dominant or left hemisphere lesions. (4) Patients with left-sided lesions may have mass effect that could impinge upon right brainstem structures. (6) • In our case, the patient had a lesion in the right cortex in the MCA • territory; however he had bipolar disorder instead of unipolar • mania disorder. Conclusions • Mood disorders following cerebrovascular accidents have required special attention because of associated functional impairment and medical morbidity. • Evaluation and pharmacological treatment may improve quality of life, especially in elderly patients. • Secondary mania is more difficult to treat than primary mania. (3,4) • Brain imaging is needed to rule out other organic causes of secondary mania, including brain tumor and head injury. (14) • Further study is needed to locate specific anatomical lesions, and to study cognitive function, treatment and other predisposing factors associated with post-stroke mania or bipolar affective disorder, including the adverse effects of medications.


















