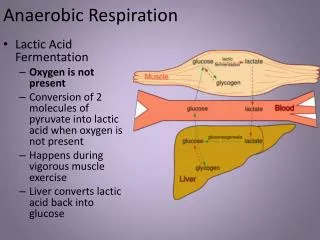
Anaerobic Bacteria
Anaerobic Bacteria. Category. Spore-forming: rod, Gram (+)--- Clostridium Nonspore-forming: see next slides . Category. Clostridium Species.

Anaerobic Bacteria
E N D
Presentation Transcript
Category • Spore-forming: rod, Gram (+)--- Clostridium • Nonspore-forming: see next slides
Clostridium Species • The clostridia are opportunistic pathogens. Nonetheless, they are responsible for some of the deadliest diseases including gas gangrene, tetanus and botulism. Less life-threatening diseases include pseudomembranous colitis (PC) and food poisoning. • cause disease primarily through the production of numerous exotoxins. • perfringens, tetani, botulinum, difficile
Clostridium Tetani Pathogenesis of tetanus caused by C tetani
General introduction • C tetani is found worldwide. Ubiquitous in soil, it is occasionally found in intestinal flora of humans and animals • C.tetani is the cause of tetanus,or lockjaw. When spores are introduced into wounds by contaminated soil or foreign objects such as nails or glass splinters
BIOCHEMICAL CHARACTERISTICS • Morphology: long and slender; peritrichous flagella,no capsule, terminal located round spore(drum-stick apperance), its diameter greater than vegetative cell. • Culture:obligate anaerobic; Gram(+); swarming occures on blood agar, faint hemolysis. • Biochemical activities:does not ferment any carbohydrate and proteins. • Resistance: tolerate boiling for 60 min.alive several ten years in soil. • Classification and Antigenic Types: C tetani is the only species. There are no serotypes 2-5 x 0.3-0.5um
No invasiveness; toxemia (exogenous infection) produces two exotoxins: tetanolysin, and tetanospasmin(a kind of neurotoxin, toxicity strong) The actions of tetanospasmin are complex and involve three components of the nervous system: central motor control, autonomic function, and the neuromuscular junction. retrograde transport to (CNS) delitescence:a few days to several weeks The two animal species most susceptible to this toxemia are horses and humans. Pathogenicity
Clostridium tetani-Tetanospasmin • disseminates systemically • binds to ganglioside receptors • inhibitory neurones in CNS • glycine • neurotransmitter • stops nerve impulse to muscles • spastic paralysis痉挛性麻痹 • severe muscle contractions and spasms • can be fatal
Clinical Manifestations • The initial symptom is cramping and twitching of muscles around a wound. The patient usually has no fever but sweats profusely and begins to experience pain, especially in the area of the wound and around the neck and jaw muscles (trismus). • Portions of the body may become extremely rigid, and opisthotonos角弓反张(a spasm in which the head and heels are bent backward and the body bowed forward) is common. • Complications include fractures, bowel impaction, intramuscular hematoma, muscle ruptures, and pulmonary, renal, and cardiac problems
Epidemiology • 1 million cases of tetanus occur annually in the world,with a mortality rate ranging from20% to 50%. But rare in most developed countries. • In some developing countries, tetanus is still one of the ten leading causes of death, and neonatal tetanus accounts for approximately one-half of the cases worldwide. • In less developed countries, approximate mortality rates remain 85% for neonatal tetanus and 50% for nonneonatal tetanus. • In the United States, intravenous drug abusers have become another population with an increasing incidence of clinical tetanus • In untreated tetanus, the fatality rate is 90% for the newborn and 40% for adults.
Immunity • Humoral immunity(antitoxin) • There is little, if any, inate immunity and the disease does not produce immunity in the patient. • Active immunity follows vaccination with tetanus toxoid
Diagnosis • Diagnosis is primarily by the clinical symptoms (above). The wound may not be obvious. • C tetani can be recovered from the wound in only about one-third of the cases. • It is important for the clinician to be aware that toxigenic strains of C tetani can grow actively in the wound of an immunized person. • Numerous syndromes, including rabies and meningitis, have symptoms similar to those of tetanus and must be considered in the differential diagnosis.
Vaccination • infant • DPT (diptheria, pertussis, tetanus) • tetanus toxoid • antigenic • no exotoxic activity
Control • The offending organism must be removed by local debridemen清创术 • toxoid • TAT; Metronidazole (For more serious wounds) • AIDS patients may not respond to prophylactic injections of tetanus toxoid
C. perfringens • soil, fecal contamination • gas gangrene • swelling of tissues • gas release • fermentation products • wound contamination
Toxins • Many of these toxins have lethal, necrotizing, and hemolytic properties; • The alpha toxin produced by all types of C. perfringens, is a lecithinase that lyses erythrocytes, platelets, leukocytes, and endothelial cells. And its lethal action is proportionate to the rate at which it splits lecithin to phosphorylcholine and diglyceride. • The theta toxin has similar hemolytic and necrotizing effects. • DNAase, hyaluronidase, a collagenase are also produced
Enterotoxin • Many strains of type A produce enterotoxin, which is a heat-labile protein and destroyed immediately at 100 ℃. • Trypsin treatment enhances the toxin activity threefold. • The toxin is produced primarily by type A strains but also by a few type C and D strains. • It disrupts ion transport in the ileum(primarily) and jejunum by inserting into the cell membrane and altering membrane permeability. • As superantigen.
Pathogenesis • Tissue degrading enzymes • lecithinase [ toxin] • proteolytic enzymes • saccharolytic enzymes • Destruction of blood vessels • Tissue necrosis • Anaerobic environment created • Organism spreads
Without treatment death occurs within 2 days • effective antibiotic therapy • debridement • anti-toxin • amputation & death is rare
Gas gangrene • Gas gangrene is a life-threatening disease with a poor prognosis and often fatal outcome. • Initial trauma to host tissue damages muscle and impairs blood supply----lack of oxygenation • Initial symptoms : fever and pain in the infected tissue.; more local tissue necrosis and systemic toxemia. Infected muscle is discolored (purple mottling) and edematous and produces a foul-smelling exudate; gas bubbles form from the products of anaerobic fermentation.
Gas gangrene • As capillary permeability increases, the accumulation of fluid increases, and venous return eventually is curtailed. • As more tissue becomes involved, the clostridia multiply within the increasing area of dead tissue, releasing more toxins into the local tissue and the systemic circulation.
Food poisoning • Enterotoxin producing strains. • These bacteria are found in mammalian faeces and soil. • Small numbers of the bacteria may also be found in foods and they may propagate rapidly to dangerous concentrations if the food is improperly stored and handled.
Food poisoning • more than 108 vegetative cells are ingested and sporulate in the gut, the toxins can act rapidly in the body, causing severe diarrhea in 6-18 hours, dysentery, gangrene, muscle infections • The action of C. perfringens enterotoxin involves marked hypersecretion in the jejunum and ileum, with loss of fluids and electrolytes in diarrhea.
Cellulitis, Fasciitis • Cellulitis, Fasciitis • Fasciitis : a rapidly progressive, destructive process in which the organisms spread through fascial plan es. • Fasciitis causes suppuration and the formation of gas • Absense of muscle involvement • rapidity
Necrotizing Enteritis • Rare, acute necrotizing process in the jejunum • Abdominal pain, bloody diarrhea, shock, and peritonitis • Mortality: 50% • Beta-toxin-producing C. perfringens type C • Septicemia
Who is at risk? • Surgical patients; patient after trauma with soil contamination. • People who ingest contaminated meat products (without proper refrigeration or reheating to inactivate endotoxin)
Epidemiology • C. perfringens type A:the intestinal tract of humans and animals, soil and water contaminated with feces. forms spores under adverse environmental conditions and can survive for prolonged periods. • Type B to E strains colonize the intestinal tract of animals and occasionally humans.
Epidemiology • Type A: gas gangrene, soft tissue infections and food poisoning • Type C: enteritis; necroticans
Laboratory identification • lecithinase production Double Hemolysis Circles
Biological Features • Anaerobic • Gram-positive • rod-shaped • sporeformer • produces a protein neurotoxic. • soil, sediments of lakes, ponds, decaying vegetation. • intestinal tracts of birds, mammals and fish.
Division ---A, B, C1, D, E, F, and G. ---type A. 62% ---Not all produce toxin. ---C and D not ---G plasmid encoded.
Transmission ---spores heat resistant. canning. anaerobic environment ---Botulism eating uncooked foods spores ---GI, duodenum, blood stream, neuromuscular synapses.
Virulence factors ---bacterial protease ---light chain,A,50 kDa; heavy chain,100kDa. ---disulfide bond. ---A potent toxin
Botulinum toxin • binds peripheral nerve receptors • acetylcholine neurotransmitter • inhibits nerve impulses • flaccid paralysis • death • respiratory • cardiac failure
Botulinum toxin • Bioterrorism • not an infection • resembles a chemical attack • 10 ng can kill a normal adult
Epidemiology ---4: foodborne, infant, wound, undetermined. ---Certain foods; wound not. ---Foodborne botulism, consumption. ---Infant botulism, 1976, under 12m. ---ingestion, colonize and produce toxin in the intestinal tract of infants. honey. ---increased. ---internationally recognized.
Clinical syndromes ---18-36 hours: ---weakness, dizziness,dryness of the mouth. ---Nausea,vomiting. ---Neurologic features: blurred vision, inability to swallow, difficulty in speech, descending weakness of skeletal muscles, respiratory paralysis.
Botulism(肉毒中毒) • food poisoning • rare • fatal • germination of spore • inadequately sterilized canned food • home • not an infection
Infection with C. botulinum • Neonatal botulism • uncommon • the predominant form of botulism • colonization occurs • no normal flora to compete • unlike adult
Wounds • extremely rare • an infection
Immunity ---specifically neutralized, antitoxin. ---toxoided, make good antigens. ---does not develop, amount toxic. ---Repeated occurrence. ---Once bound, unaffected by antitoxin. ---circulating toxin ,neutralized , injection of antitoxin. ---treated immediately with antiserum. ---multivalent toxoid,unjustified,infrequency. experimental vaccine.
Diagnosis ---by clinical symptoms alone ---differentiation difficult. --- most direct and effective: serum or feces. ---most sensitive and widely used: mouse neutralization test. 48h. Culturing of specimens 5-7d.
Treatment • Individuals known to have ingested food with botulism should be treated immediately with antiserum. • antibiotic therapy (if infection) • Vaccination will not protect hosts from botulism, however passive immunisation with antibody is the treatment of choice for cases of botulism.