Download

1 / 32
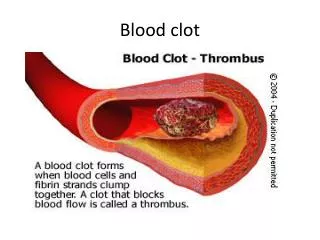
320 likes | 634 Vues
To Clot Or Not To Clot… Emergency Care for Coagulation Disorders/Conditions. Kay Decker Hemophilia Nurse Coordinator Hamilton Niagara Regional Hemophilia Program McMaster Children’s Hospital Current Concept in Pediatrics October 16 th , 2009. Our Program.

E N D
To Clot Or Not To Clot…Emergency Care for Coagulation Disorders/Conditions Kay Decker Hemophilia Nurse Coordinator Hamilton Niagara Regional Hemophilia Program McMaster Children’s Hospital Current Concept in Pediatrics October 16th, 2009
Our Program Responsible for all patients (Adult/Peds) with hemophilia and other bleeding disorders such as rare factor deficiencies and vWD.
Objectives • Hemophilia Basics • Hemophilia Emergency Care • Key Points • Summary
What is Hemophilia? Hemophilia • A genetic (inherited) disorder in which a clotting protein is missing or deficient causing prolonged bleeding Hemophilia A Factor VIII Deficiency Classic Hemophilia Hemophilia B Factor IX Deficiency Christmas Disease
Incidence • Factor VIII deficiency (Hemophilia A) • affects 1 in 10,000 males (www.ahcdc.org : CHR) • 60% have severe disease • Factor IX deficiency (Hemophilia B) • affects 1 in 25,000 to 30,000 males (www.ahcdc.org : CHR) • 50% have severe disease • 2,400 affected males across Canada • Affects all races, all social classes • X-linked inheritance • 1/3 of FVIII and 1/5 of FIX cases are “spontaneous” with no family history
Characteristics of Hemophilia by Severity *clotting factor activity in a normal person is said to be 100%, ranging anywhere from 50-150%
Hemophilia is: • low or absent factor VIII (8) or factor IX (9) • curable • bleed really fast • carried on the y chromosome
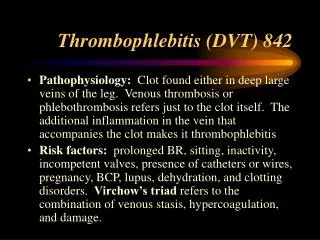
Serious Joints (hemarthrosis) Muscle/soft-tissue Mouth/gums/nose Hematuria Life-threatening CNS Gastrointestinal Neck/throat Severe trauma Bleeding Manifestations in Hemophilia
Lacerations and Cuts • Superficial cuts • apply pressure • normal first aid • Deep lacerations • factor replacement before sutures and removal of sutures • Head trauma interventions, if appropriate
Mucous Membrane Bleeding • Frenulum tears / mouth injuries • Tooth loss & eruption / dental work • Epistaxis (nosebleeds)
The assessment of hemarthrosis is difficult in young children. If you suspect that a child is having a knee bleed. What would your Immediate assessment include? • X-ray to determine the severity of the bleed • Early factor replacement before investigations • RICE • Attempt to manipulate the joint to improve range
Limb Compartments • Bleeding into the iliopsoas, anterior calf and forearm are high risk for compartment syndrome • As the muscle expands nerves and vessel are compressed • Permanent disability can occur if prompt treatment is not given
How Do We Treat Hemophilia? • Factor replacement – Recombinant FVIII or Recombinant FIX • DDAVP (for mild only FVIII) – helps increase endogenous levels of FVIII • Anti-fibrinolytics (Tranexamic acid) • RICE (Rest, Ice, Compression, Elevation) • Comprehensive care – bleed prevention
Key Points • FACTOR FIRST, diagnostic investigations later • Factor is $$$; the entire vial should be used or waste should be minimized • NO invasive procedures without first replacing missing factor • NO IM injection • NO ASA containing products • ½ life of VIII is 8-12hours • ½ life of FIX is 18-24hours • Allergies to factor concentrate are rare • Patients are instructed to keep records • Good healthy veins (Lifeline)
When performing venipuncture on a patient with hemophilia. What are some nursing considerations? • Hold the site uninterrupted for 5 minutes • Dig around the vein if the patient has difficult venous access to minimize the amount of pokes • Use the smallest gauge needle as possible • a & c
The Evaluation of Cases According to Most Urgency to Least Urgent Canadian Paediatric Triage and Acuity Scale: Implementation Guidelines for Emergency Departments
Triage of Bleeding Disorders HHS clinical guidelines supports: • “All hemophiliac patients will be triaged as CTAS II” (statement found on HHS intranet/Emergency Medicine/Physician Clinical Guidelines) Ref: M.Bullard et al., CJEM,March 2008; 10(2), p 132-146; Warren, et al. CJEM, May 2008; 10(3). p 224-232 )
Case Study A 10 year old male severe hemophilia B patient comes into the ER Department crying with a swollen knee after playing baseball.
Management: Joint Injury • Triage Level II (Emergent) seen within 15 minutes • Is this a life-threatening incident? No! But bleeding into a joint can cause permanent joint damage even after the 1st bleed and is very painful (the amount of bleeding into the joint will determine the amount of damage to the joint). • Identify type and severity of bleeding disorder • If and when he last had a treatment • Treat ASAP • Diagnostic test later • Notify the hematologist on call • Instruct the patient or family to notify the HTC for follow-up
Summary If a child with hemophilia states that he has a bleed… believe.
Summary 85% of treatments are given by patients or caregivers so when a patient comes to ER it should be a warning of something unusual and potentially dangerous. Dr. I. Walker…
Summary • Early and appropriate treatment of each bleeding episode is critical to minimize complications. Replacement of deficient clotting factor is the single most important step in ANY intervention.
SUMMARY If in doubt… FACTOR FIRST.
What are some general principles of care? • Prevention of bleeding is the goal • When in doubt treat!! • Acute bleeds should be treated as early as possible • All of the above
Comprehensive Care Team Our program provides service for Pediatric and Adult population Team: • Dr. Chan (Pediatric Director) • Dr. Walker (Adult Director) • Dr. Webert (Adult Hematologist) • Kay Decker (Hemophilia Nurse Coordinator) • Rebecca Goldsmith (Pediatric Thrombosis/Hemophilia Nurse) • Theresa Almonte (Program Secretary) • Cecily Bos (PT) • Linda Waterhouse (Pediatric SW)
Additional Information • www.machealth.ca • www.hemophilia.ca • www.wfh.org • www.ahcdc.org