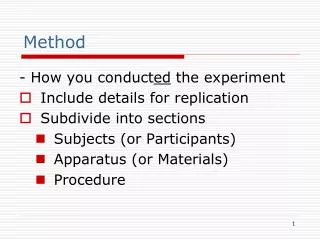
Method
Method. Two month data collection period (Feb-Mar 2004) NHS and independent hospitals in England, Wales, N Ireland, Guernsey, Isle of Man and Defence Secondary Care Agency Adults >=16 years of age Open repair; endovascular repair; diagnosed but not treated and died in hospital. Method (cont).

Method
E N D
Presentation Transcript
Method • Two month data collection period (Feb-Mar 2004) • NHS and independent hospitals in England, Wales, N Ireland, Guernsey, Isle of Man and Defence Secondary Care Agency • Adults >=16 years of age • Open repair; endovascular repair; diagnosed but not treated and died in hospital
Method (cont) • Expected sample size was 1129 operated cases and 106 non-operated cases • Questionnaire sent to combination of surgeon, anaesthetist and radiologist • No casenote review • Organisational questionnaire for each hospital • Risk stratification planned using a published model • Multidisciplinary advisory group
Data overview – hospital participation • 226 hospitals identified as possibly undertaking AAA repair • 188 completed organisational questionnaires • 181 eligible to take part in study (163 NHS and 18 independent) • 87% participation rate for clinical questionnaires
Size of vascular unit • Large • 500,000 patients, 4 surgeons, potential for vascular surgical on-call rota • Intermediate • <500,000 patients, fully equipped for vascular surgery, not enough surgeons for on-call rota • Remote • Remote, small catchment population
Recommendation Trusts should ensure the availability outside normal working hours of radiology services including CT scanners.
Published evidence • Improved outcomes for unruptured AAA when higher volumes performed by: • surgeons • hospitals • US recommendation – hospitals should perform 50 cases/year • 19/181 hospitals in this study performed 50 or more cases/year
Recommendation Clinicians, purchasers, Trusts and Strategic Health Authorities should review whether elective aortic aneurysm surgery should be concentrated in fewer hospitals.
Vascular anaesthetic on-call rotas • 3% (5/178) of hospitals reported that they had an anaesthetic on-call rota for vascular surgery • Should large vascular units implement anaesthetic vascular on-call rotas?
Use of recovery areas after elective surgery • 4 hospitals reported that the recovery area was the preferred destination • 9% of elective patients were reported to have been cared for in recovery areas for a substantial period of time (from the anaesthetic questionnaire)
Recommendation Major elective surgery should not take place unless all essential elements of the care package are available.
Outcome of elective open repair Overall mortality was 6.2%
Outcome after emergency admission with ruptured AAA, all patients
Palliative care vs. operation on emergency admission with AAA
Outcome after emergency admission with unruptured AAA, all patients
Patient information • How much information should be given to patients on the organisation of vascular services? • How should this information be provided?
Cancellations • 1 in 25 patients cancelled because no ward bed • 1 in 6 patients cancelled because no critical care bed
Recommendation Patients with an aortic aneurysm requiring surgery must have equal priority with all other patients with serious clinical conditions for diagnosis, investigation and treatment.
Recommendation Trusts should take action to improve access to Level 2 beds for patients undergoing elective aortic aneurysm repair so as to reduce the number of operations cancelled and inappropriate use of Level 3 beds.
Comorbidities • Cardiac history and signs associated with increased risk of death • Diabetes carried no additional risk of death in this study • Increased risk of death among morbidly obese or cachectic patients
Recommendation Trusts should ensure that clinicians of the appropriate grade are available to staff preoperative assessment clinics for aortic surgery patients.
Specialty of surgeon <1% 25% 75%
Postoperative complications within 30 days of surgery • 21% had an infective complication, most commonly of the chest and wound • 7% had a myocardial infarct, nearly half these patients died
Emergency surgery • Unscheduled admission
Comorbidities • Higher risk of death in patients with cardiac disease, diabetes, morbid obesity or cachexia • Mortality increased among patients not fully conscious, though 2/7 patients with GCS below 9 did survive