Download
1 / 24
260 likes | 808 Vues
Status of the Trial for Thymectomy in Nonthymomatous MG Patients Receiving Prednisone (MGTX). Henry J. Kaminski Department of Neurology & Psychiatry Saint Louis University. Outline. Rationale for the MGTX trial Trial structure What has been learned The near future.

E N D
Status of the Trial for Thymectomy in Nonthymomatous MG Patients Receiving Prednisone (MGTX) Henry J. Kaminski Department of Neurology & Psychiatry Saint Louis University
Outline • Rationale for the MGTX trial • Trial structure • What has been learned • The near future
Evidence Based Review • Evidence-based AAN Practice Parameter • 28 Class II studies (Class II. Evidence provided by well-designed observational studies with concurrent controls, e.g., case–control and cohort studies), published between 1953-1998 • 21 MG cohorts • 4136 surgical pts; 4354 non-surgical pts • Majority used transsternal approach • F/U mean range 3-28 years • No blinded assessments
AAN Practice Parameter • Conclusions and recommendations • Benefit of thymectomy not established conclusively • Recommended as treatment option • Controlled trial needed
History of MGTX • October 2000 at the American Neurological Association 1st Investigator Meeting organized by John Newsom-Davis • Gil Wolfe receives Muscular Dystrophy Association (USA) funds for planning process • First submission to the National Institutes of Health (February 1, 2001) and Medical Research Council
History of MGTX • Fourth submission to the National Institutes of Health (November 15, 2004) • Funding approved (September 2005) • Final protocol revisions performed in collaboration with the NIH • NIH supports Biomarker Ancillary Study (March 2006)
Thymectomy trial in non-thymomatous MG patients on prednisone (1R01 NS42685) Present Leadership Gil Wolfe, MD (Study Chair) Gary Cutter, PhD (Director, DCC,) Immaculada Aban, PhD (Deputy Director, DCC) Henry Kaminski, MD (Director Biomarker study, Study Vice Chair) Alfred Jaretzki, MD (Surgical Chair) Greg Minisman (Project Manager)
History of MGTX • March 2006 Training meetings held in San Francisco and Oxford • April 2006 first center obtains full regulatory approval • July 2006 first patient randomized
MGTX Protocol Inclusion criteria AChR binding Ab pos (≥0.5) MGFA Class 2-4; disease duration < 5 years Age at least 18 and < 65 years Optimal anti-cholinesterase dose Prednisone naïve or not Main exclusion criteria Previous thymectomy or sternotomy or thoracotomy Immunosuppressive therapy (x prednisone) within last year Rituximab at any time Medically or psychiatrically unfit for thymectomy Chest CT or MR evidence of thymoma Pregnancy or lactation, or considering becoming pregnant Current prednisone > 0.75 mg/kg or 50 mg/d (or ADequivalent)
MGTX Trial RANDOMIZATION Surgery prednisone 1.5 mg/kg AD prednisone 1.5 mg/kg AD Minimal Manifestations prednisone taper Minimal Manifestations prednisone taper 1° Composite AUQTC and AUDTC, at 3 years 2° prednisone AUDTC at 1,2 years Time to Minimal Manifestations ∆QMG, MG-ADL at 1,2,3 years ∆SF-36 at 1,2,3 years hospital days at 2, 3 years outcome measures
MGTX Protocol Composite primary outcome Prednisone requirements (AUDTC-Area Under the Dose Time Curve) Clinical response (AUQMGTC) Blinded evaluator (BE) Study specific adverse events
Sample Size • 90% power, P=0.05, AUDTC at 3 years is 30% of the baseline mean, the trial requires 60 subjects in each arm or 120 total. • 20% dropouts over 3 years yields a sample size of 75 per group or a 150 total. • In order to provide a reasonable test of the effect for those pre-medicated with prednisone versus those not on prednisone, sample size increased to 100 per group. This allows for approximately 50 patients in each subgroup. For the 30% difference, 50 patients would yield a power of 84% within each subgroup. Total Sample Size of 200.
MGTX Protocol • Minimal Manifestation Status (MGFA CriteriaNeurology 2000;55:16) • No symptoms or functional limitations from MG but some weakness present on careful examination • QMG score <14; ≤ baseline value • Treatment options • Azathioprine or other IS agent allowed • if MMS not reached by 1 year OR severe prednisone-related AEs via protocol deviation
Biomarker Ancillary Study Identify biomarkers (genes or proteins) associated with the diagnosis of MG SNP, genomic profile, proteomic profile, autoAb profile, thymic pathology Angela Vincent Alex Marx and Philip Strobel Identify biomarkers through genomic and proteomic profiling associated with clinical parameters Identify biomarkers associated with thymic pathology as assessed by tissue array profiling
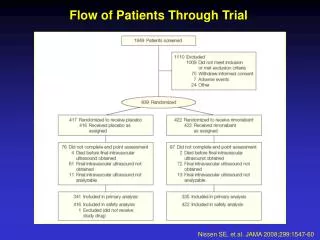
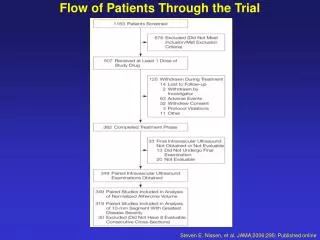
Patient Screening and Randomization • 5,760 patients (3,162 from centers outside the US) and 2,430 from US Centers) as of September 2009 • 170 eligible patients • 89 refused • 81 randomized (19 from US Centers) • 69% of eligible US patients refused while 44% of eligible patients outside the US refused.
Randomized Patients • 58% are women • Mean age: 34 years, sd 11.68 • Class II 64% • Class III 33% • Class IV 3% • DROP OUTS 5 Patients-much lower than expected
Leading Centers • Buenos Aires, Argentina (Claudio Mazia, PI) 14 patients • Santiago, Chile (Gabriel Cea) 7 patients • Vancouver, British Columbia, Canada (Joel Oger) 7 patients • Cape Town, South Africa (Jeannine Heckmann) with 5 patients.
MGTX Challenges • Regulatory clearance • US sites: 9.67 ± 0.74 months • Non-US sites: 13.4 ± 0.96 months • p=0.0175 • IRB/EC approval • US sites: 4.4 months • Non-US sites: 5.3 months • Subcontract approval • US sites: 7.86 months • Non-US sites: 8.65 months • Native language translations • Insistence on local currency Aban et al. J Neuroimmunol 2008; 201-202:80-84
MGTX Challenges • IRB/Ethics committees • Local practices (Italy and birth control) • MREC approval in UK • Japan, Netherlands, Taiwan, UK would not permit use of prednisone originating in US • Federalwide Assurance (FWA) • Via US Office of Human Research Protections of DHHS • Non-US administrators may not be fluent in English • Renewal q3 yrs • US State Dept. clearance • S. America, Asia delays (17 mos for Brazil) • Training and certification • Now done locally by Project Manager • Certification tests for neurologists and surgeons • Data Entry System certification
John Newsom-Davis (1932-2007) The Leadership Team, colleagues at the NIH, and all participating investigators continue to work towards successful completion.