Download
1 / 16

E N D
1. Alternate Level of Care Beyond Beds This evening�s presentation is aimed at providing the Board and our community with a better understanding of the bed crisis that has been facing our community for more than two years.
This evening�s presentation is aimed at providing the Board and our community with a better understanding of the bed crisis that has been facing our community for more than two years.
2. ALC � A Definition Complex issue extending beyond hospital
ALC represents multitude of patient populations all requiring different care
ALC = patients who no longer require hospital care, but cannot be discharged due to lack of beds/resources in community
Not receiving the right care in the right place The Alternate Level of Care issue -- better known as ALC -- is extremely complex and extends far beyond the walls of the hospital. Adding to the complexity is the fact that ALC can represent a multitude of patient populations, all requiring different types of care.
It is generally understood that ALC patients are patients who no longer require hospital care but cannot be discharged due to a lack of beds and/or resources in the community. In short, ALC patients are not receiving the right care in the right place. The Alternate Level of Care issue -- better known as ALC -- is extremely complex and extends far beyond the walls of the hospital. Adding to the complexity is the fact that ALC can represent a multitude of patient populations, all requiring different types of care.
It is generally understood that ALC patients are patients who no longer require hospital care but cannot be discharged due to a lack of beds and/or resources in the community. In short, ALC patients are not receiving the right care in the right place.
3. The Faces of ALC The majority of ALC patients require long-term care beds
Other placement/services for ALC patients:
Convalescent Care
Rehabilitation centre/beds
Palliative care
Mental Health bed/services/facility
Home care/supportive housing
Acquired Brain Injury support/services
The large majority of ALC patients are awaiting placement in a long term care facility. They typically represent over 50% of a hospital�s ALC population.
About 25% of ALC patients are patients requiring convalescent care
But there are a significant number of ALC patients who require different types of care services to help them recover from their illness or injuries. ALC patients may also be waiting for the following placement and/or services:
Rehabilitation centre or bed
Palliative care bed
Mental health bed / services
Addiction facility
Home care / supportive housing
Acquired Brain Injury support / services
The large majority of ALC patients are awaiting placement in a long term care facility. They typically represent over 50% of a hospital�s ALC population.
About 25% of ALC patients are patients requiring convalescent care
But there are a significant number of ALC patients who require different types of care services to help them recover from their illness or injuries. ALC patients may also be waiting for the following placement and/or services:
Rehabilitation centre or bed
Palliative care bed
Mental health bed / services
Addiction facility
Home care / supportive housing
Acquired Brain Injury support / services
4. ALC � Community Based Services Community support services expected and required for seamless system of care:
Long-term care facilities
Convalescent care beds
Rehabilitation facilities/support services
Palliative care services
Mental Health facilities/community-based services
Supportive care/supportive housing
Independent living services
Complex continuing care beds/services The multiplicity of support services one should expect to find in a community to ensure an appropriate and seamless system of care would typically include:
Long term care facilities
Convalescent care beds
Rehabilitation facilities / support services
Palliative care services
Addiction centres / outreach services
Mental health facilities / community-based support services
Supportive care
Supportive housing
Home care services
Independent living services
Complex continuing care beds / servicesThe multiplicity of support services one should expect to find in a community to ensure an appropriate and seamless system of care would typically include:
Long term care facilities
Convalescent care beds
Rehabilitation facilities / support services
Palliative care services
Addiction centres / outreach services
Mental health facilities / community-based support services
Supportive care
Supportive housing
Home care services
Independent living services
Complex continuing care beds / services
5. Community-Based Support �City of Greater Sudbury City of Greater Sudbury�s community-based health support services:
Insufficient long-term care capacity
Insufficient convalescent care capacity
Significant lack of home care services
Significant lack of rehabilitation services
Significant lack of supportive housing
Lack of mental health community-based services
While there are bright spots such as the capital expansion project underway for Maison La Paix House, the City of Greater Sudbury�s health and social support services have proven inadequate to serve the community�s needs.
We have insufficient long-term care and convalescent care capacity coupled with a significant lack of home care, rehabilitation and outreach services as well as supportive housing.
It should be noted that last year the Regional Office of the MOHLTC facilitated a local area planning committee comprised of community representatives. The committee completed a gap analysis for our district. The results have note yet been released but we expect they will be consistent with the broader provincial system recommendations.While there are bright spots such as the capital expansion project underway for Maison La Paix House, the City of Greater Sudbury�s health and social support services have proven inadequate to serve the community�s needs.
We have insufficient long-term care and convalescent care capacity coupled with a significant lack of home care, rehabilitation and outreach services as well as supportive housing.
It should be noted that last year the Regional Office of the MOHLTC facilitated a local area planning committee comprised of community representatives. The committee completed a gap analysis for our district. The results have note yet been released but we expect they will be consistent with the broader provincial system recommendations.
6. Regional Challenges ALC a provincial and national health care issue
Unique regional challenges that compound ALC issue for the north:
Older, less healthy population
Youth migration
Vast geographic dispersion
Economically depressed area
While the ALC issue is a problem that can be found throughout the province and Canada, there are some challenges that are unique to our region. These challenges include:
- an older, less healthy population;
youth migration;
vast geographic dispersion; and
- an economically depressed area where for many a government funded health care facility is the only option.While the ALC issue is a problem that can be found throughout the province and Canada, there are some challenges that are unique to our region. These challenges include:
- an older, less healthy population;
youth migration;
vast geographic dispersion; and
- an economically depressed area where for many a government funded health care facility is the only option.
7. Population Health in the North Northeastern Ontario residents less healthy on almost all indicators
Advances in care mean people live longer, but with higher number of dependant years
Challenges of providing care to elderly exacerbated by poorer health
Impact of an aging and less healthy population felt more acutely
On almost all indicators, people in northeastern Ontario are less healthy than their southern counterparts.
We have higher incidence of cancer, heart disease, stroke and debilitating illnesses such as diabetes or degenerative bone disease. We also have higher rates of injury due to accidents.
Because we tend to be less healthy, the impact of a nation-wide aging population is felt more acutely in northeastern Ontario. This is due in part to the fact that with advances in care, people in general tend to live longer, but also have a higher number of dependant years. The challenges of providing care for people in their dependant years is exacerbated by poor health.
We are already dealing with these issues at the Sudbury Regional Hospital where we have concrete data that shows a consistent increase in the intensity of patients receiving care at our hospital.On almost all indicators, people in northeastern Ontario are less healthy than their southern counterparts.
We have higher incidence of cancer, heart disease, stroke and debilitating illnesses such as diabetes or degenerative bone disease. We also have higher rates of injury due to accidents.
Because we tend to be less healthy, the impact of a nation-wide aging population is felt more acutely in northeastern Ontario. This is due in part to the fact that with advances in care, people in general tend to live longer, but also have a higher number of dependant years. The challenges of providing care for people in their dependant years is exacerbated by poor health.
We are already dealing with these issues at the Sudbury Regional Hospital where we have concrete data that shows a consistent increase in the intensity of patients receiving care at our hospital.
8. Economic Factors in the North Lower socio-economic status leads to poorer health
Northeastern Ontario economically depressed area creates two-fold problem:
Lack of resources to pay for retirement home, government-subsidized LTC facility only option
With youth migration, many unable to return to provide care when parents become elderly or infirm People of lower socio-economic status are less healthy in general, leading to greater incidence of illness requiring care. As an economically depressed area our problem is two-fold:
Many people of advancing years lack the resources necessary to pay for a retirement home, opting instead for a government subsidized long-term-care facility. As a consequence, many retirement home beds in the community sit idle while people wait for a bed which is geared to their income.
High unemployment rates have led to an out-migration of our youth who must seek employment in other areas. As a result, many are unable to return to their community of origin to provide care when their parents become elderly or infirm. People of lower socio-economic status are less healthy in general, leading to greater incidence of illness requiring care. As an economically depressed area our problem is two-fold:
Many people of advancing years lack the resources necessary to pay for a retirement home, opting instead for a government subsidized long-term-care facility. As a consequence, many retirement home beds in the community sit idle while people wait for a bed which is geared to their income.
High unemployment rates have led to an out-migration of our youth who must seek employment in other areas. As a result, many are unable to return to their community of origin to provide care when their parents become elderly or infirm.
9. ALC and Long Term Care Majority of ALC patients waiting for long-term-care
Ministry guidelines allow for ALC patients to wait in hospital until a LTC bed of their choice becomes available
Can be a lengthy wait, impacting hospital operations
When hospital acute and surgical care affected by ALC, Ministry can invoke Crisis 1-A designation
Earlier, I provided you with a glimpse of the many faces of ALC and I demonstrated that the issue of ALC extends beyond just long term care. However, as the majority of ALC patients in our community are waiting for a bed in a LTC facility, it remains a huge challenge which must be addressed.
According to established Ministry guidelines, ALC patients requiring placement in a Long Term Care facility can wait in hospital until a LTC bed of their choice becomes available. This can be a lengthy wait, impacting the daily operations of a hospital.
When the daily operations of the hospital are impacted to such a degree that the ability to provide acute and surgical care services becomes threatened, the province can invoke a Category 1-A Crisis Designation. Earlier, I provided you with a glimpse of the many faces of ALC and I demonstrated that the issue of ALC extends beyond just long term care. However, as the majority of ALC patients in our community are waiting for a bed in a LTC facility, it remains a huge challenge which must be addressed.
According to established Ministry guidelines, ALC patients requiring placement in a Long Term Care facility can wait in hospital until a LTC bed of their choice becomes available. This can be a lengthy wait, impacting the daily operations of a hospital.
When the daily operations of the hospital are impacted to such a degree that the ability to provide acute and surgical care services becomes threatened, the province can invoke a Category 1-A Crisis Designation.
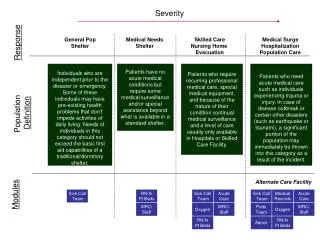
10. Crisis 1-A Designation Category 1-A Crisis: ALC patients awaiting LTC placement in hospital are required to accept the first appropriate level of care bed available, while they wait for their bed of choice.
In April 2004, the Ministry of Health and Long-Term Care granted a Category 1-A Crisis Designation for all ALC patients at HRSRH Category 1-A Crisis designation means that ALC patients awaiting LTC placement in hospital are required to accept the first appropriate level of care bed available within the city, regardless of the facility, while they wait for their bed of choice. Presently, the HRSRH is operating under a Category 1-A Crisis designation.
Expanded Category 1-A Crisis designation means that ALC patients awaiting LTC placement in hospital are required to accept the first appropriate level of care bed available within the entire district as defined by the Ministry.
Last year, the HRSRH was operating under this expanded designation because there were no LTC beds available within the City of Greater Sudbury. The expanded designation included the communities of Espanola and Manitoulin Island. Although Chapleau is also within the district, the transfer of patients to that community was eliminated by the Ministry.
A significant community impact of the Crisis 1-A designation that should be noted is that it effectively blocks any other means of admission to a LTC facility. Residents waiting for a LTC bed from their homes are provided with a one-week window each month, when the Crisis designation is lifted.Category 1-A Crisis designation means that ALC patients awaiting LTC placement in hospital are required to accept the first appropriate level of care bed available within the city, regardless of the facility, while they wait for their bed of choice. Presently, the HRSRH is operating under a Category 1-A Crisis designation.
Expanded Category 1-A Crisis designation means that ALC patients awaiting LTC placement in hospital are required to accept the first appropriate level of care bed available within the entire district as defined by the Ministry.
Last year, the HRSRH was operating under this expanded designation because there were no LTC beds available within the City of Greater Sudbury. The expanded designation included the communities of Espanola and Manitoulin Island. Although Chapleau is also within the district, the transfer of patients to that community was eliminated by the Ministry.
A significant community impact of the Crisis 1-A designation that should be noted is that it effectively blocks any other means of admission to a LTC facility. Residents waiting for a LTC bed from their homes are provided with a one-week window each month, when the Crisis designation is lifted.
11. Impact of ALC at HRSRH ALC has domino effect on hospital system
Hospital needs regular flow of patients moving out
When outflow does not occur:
Emergency Department overcrowding
Surgical Cancellations
Impact on resources (human, financial, utilization)
The ALC issue is a system issue which has a domino effect on almost every facet of the organization. For a hospital to run smoothly there must be a regular flow of patients moving out of the system once they have completed their acute phase of care. When this outflow does not occur, it creates several difficulties for the hospital including:
Overcrowding in the Emergency Department
Surgical cancellations
Impact on resourcesThe ALC issue is a system issue which has a domino effect on almost every facet of the organization. For a hospital to run smoothly there must be a regular flow of patients moving out of the system once they have completed their acute phase of care. When this outflow does not occur, it creates several difficulties for the hospital including:
Overcrowding in the Emergency Department
Surgical cancellations
Impact on resources
12. Impact of ALC at HRSRH Emergency Department Overcrowding:
Most acute symptom of the problem
Patients must wait in the ED until a bed becomes available
Twelve or more admitted patients waiting in ED triggers Level Three Status
When capacity is reached, physicians do not have beds in which to examine or treat patients
Creates long wait times in the ED
Very stressful for both staff and patients
Emergency Department overcrowding
Emergency Department overcrowding is the most acute symptom of the problem. Patients who are admitted to the hospital, but cannot be given a bed, must stay in the ED until one becomes available. Twelve or more admitted patients is referred to as Level Three Status.
When Emergency Department capacity is reached, physicians do not have beds in which to place patients for examination. The Emergency Department must still deal with critical patients when they arrive. As a consequence, patients with less severe complaints must often wait for long periods of time. This results in a great deal of stress for both staff and patients.
The impact on the working environment in the ED is significant. The workload for our nurses and physicians is difficult and highly stressful. I want to take this opportunity to recognize their efforts and thank them on behalf of the Board and the community.Emergency Department overcrowding
Emergency Department overcrowding is the most acute symptom of the problem. Patients who are admitted to the hospital, but cannot be given a bed, must stay in the ED until one becomes available. Twelve or more admitted patients is referred to as Level Three Status.
When Emergency Department capacity is reached, physicians do not have beds in which to place patients for examination. The Emergency Department must still deal with critical patients when they arrive. As a consequence, patients with less severe complaints must often wait for long periods of time. This results in a great deal of stress for both staff and patients.
The impact on the working environment in the ED is significant. The workload for our nurses and physicians is difficult and highly stressful. I want to take this opportunity to recognize their efforts and thank them on behalf of the Board and the community.
13. Impact of ALC at HRSRH Surgical Cancellations:
When system capacity is reached and no other options are available, hospital is forced to cancel elective surgery
To minimize impact on patients:
surgeries rescheduled within two week timeframe
Fewer procedures scheduled during peak times
Results in increased waits for surgical procedures Surgical Cancellations
When system capacity is reached and no other options are available, as a last resort the hospital is forced to cancel elective surgery.
In order to minimize the impact that these cancellations have on patients, the hospital strives to reschedule their surgeries within a two-week period. The hospital may also schedule fewer procedures during peak demand times to avoid cancellations.
Both situations have the consequence of increased waits for surgical procedures and could ultimately impact the hospital�s ability to meet Ministry Wait Time Strategy targets.Surgical Cancellations
When system capacity is reached and no other options are available, as a last resort the hospital is forced to cancel elective surgery.
In order to minimize the impact that these cancellations have on patients, the hospital strives to reschedule their surgeries within a two-week period. The hospital may also schedule fewer procedures during peak demand times to avoid cancellations.
Both situations have the consequence of increased waits for surgical procedures and could ultimately impact the hospital�s ability to meet Ministry Wait Time Strategy targets.
14. Impact of ALC at HRSRH Impact on resources:
Human Resources: Expending valuable resources reacting to and planning for bed crisis, creating stressful working environment for physicians and staff
Utilization: ALC leads to increase in expected length-of-stay, impacting hospital efficiency
Financial: HRSRH has borne the cost of keeping extra beds open and staffed, and has not been able to make full use of targetted wait time and priority program funding.
Impact on Resources
Human Resources: When operating at a Level Three Status, staff and physicians on all medical floors are required to determine whether there are patients ready for discharge or transfer in order to accommodate acute care patients coming into the hospital system. The hospital must expend valuable resources reacting to and planning for this situation on a regular basis. It also creates a very stressful working environment for our staff and physicians.
Utilization: ALC pressures have resulted in an increase in conservable days (days exceeding expected length of stay in hospital) which may have an impact on the hospital�s efficiency rating and subsequent funding. Almost all conservable days are attributable to the ongoing ALC crisis.
Financial: In order to cope with the bed crisis during the summer period, the HRSRH opened thirteen surgical beds. In addition, in May 2005, the hospital opened five medical beds and these beds remain open. Unless recouped, this cost must be absorbed in the hospital�s global budget. The hospital has also had to engage a non-urgent patient transport service because the City of Sudbury�s ambulance service has limited to no capacity for non-urgent transport.Impact on Resources
Human Resources: When operating at a Level Three Status, staff and physicians on all medical floors are required to determine whether there are patients ready for discharge or transfer in order to accommodate acute care patients coming into the hospital system. The hospital must expend valuable resources reacting to and planning for this situation on a regular basis. It also creates a very stressful working environment for our staff and physicians.
Utilization: ALC pressures have resulted in an increase in conservable days (days exceeding expected length of stay in hospital) which may have an impact on the hospital�s efficiency rating and subsequent funding. Almost all conservable days are attributable to the ongoing ALC crisis.
Financial: In order to cope with the bed crisis during the summer period, the HRSRH opened thirteen surgical beds. In addition, in May 2005, the hospital opened five medical beds and these beds remain open. Unless recouped, this cost must be absorbed in the hospital�s global budget. The hospital has also had to engage a non-urgent patient transport service because the City of Sudbury�s ambulance service has limited to no capacity for non-urgent transport.
15. Potential ALC Solutions Create capacity for long-term and convalescent care
Create capacity for full spectrum of community supports (home care, supportive care ,supportive housing, improved addictions and mental health services)
Improved respite care and supports for family members who choose to care for elderly or infirm people in their homes
Implement strategies to make more efficient use of resources i.e. Nursing Outreach Strategy to re-direct patients from ED
Reduce financial barriers to accessing retirement homes Some potential solutions may be:
Reduce financial barriers to accessing retirement homes.
Create capacity not only for long-term care, but also for the full spectrum of community supports necessary -- home care, increased supportive care for those with brain or other debilitative injuries, improved addictions and mental health services, etc.
Create capacity for convalescent care so that health issues of a long term but not permanent nature do not result in permanent residence in LTC facilities.
Improve respite care and supports for family members who choose to care for elderly or infirm people in their homes.Some potential solutions may be:
Reduce financial barriers to accessing retirement homes.
Create capacity not only for long-term care, but also for the full spectrum of community supports necessary -- home care, increased supportive care for those with brain or other debilitative injuries, improved addictions and mental health services, etc.
Create capacity for convalescent care so that health issues of a long term but not permanent nature do not result in permanent residence in LTC facilities.
Improve respite care and supports for family members who choose to care for elderly or infirm people in their homes.
16. ALC Future Outlook As Baby Boomers age ALC problem will grow
Need to take control of our own health
Must improve preventative and wellness strategies
Education and personal and community planning is key The problem will continue to grow as the Baby Boomers age, and we do bear some of the responsibility.
It is incumbent upon us to take control of our own health. As we grow older, we must grow older in a healthier manner to reduce the impact on our universal health care system. We must improve preventative sand wellness strategies to prevent hospitalization.
We must take control of our future. Education and planning for the eventuality of poor health and the inevitable aging we will experience is key to maintaining dignity and retaining the ability to make our own decisions.
The problem will continue to grow as the Baby Boomers age, and we do bear some of the responsibility.
It is incumbent upon us to take control of our own health. As we grow older, we must grow older in a healthier manner to reduce the impact on our universal health care system. We must improve preventative sand wellness strategies to prevent hospitalization.
We must take control of our future. Education and planning for the eventuality of poor health and the inevitable aging we will experience is key to maintaining dignity and retaining the ability to make our own decisions.