Download
1 / 39
390 likes | 580 Vues
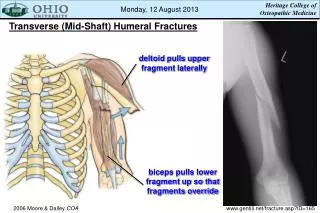
STD UPDATE Bryan Larsen, PhD Marian University College of Osteopathic Medicine. Here Lies Penicillin. “TET” A great run 1985. Sulfa 1945. Z Max 20??. 1980. Spec Tino My Cin 1975. Cefixime Ceftriaxone 20??. Cipro Died Age 10. Arrived January 2011. Education/ Counseling.

E N D
STD UPDATE Bryan Larsen, PhD Marian University College of Osteopathic Medicine
Here Lies Penicillin “TET” A great run 1985 Sulfa 1945 Z Max 20?? 1980 Spec Tino My Cin 1975 Cefixime Ceftriaxone 20?? Cipro Died Age 10
Education/ Counseling Age Groups STD Clinical Infection Behaviors High Risk Groups Prevention Strategy Immuno-prophylax STI Subclinical Infection Ed/SES Culture Population Diversity Geography Antibody Tests Diagnostic Options Genetics Molecular Technol. History Risk Profile Organism Diversity Epidemiolog Synergy Bacteria Treatment Behaviors Virus Efficacy Fungi Protozoon Metazoon Resistance
Alphabet Soup PID HCV HBV GC TORCH MG HIV HPV TRICH BV HSV CT HAV
CDC STDTG Areas of Emphasis Prevention (everyone participates) Populations (special risks) Particulars (11 new key recommendations)
Prevention In the hands of the physician and the patient
Prevention Strategies Identify asymptomatic infected and symptomatic unlikely to seek treatment Effective diagnosis and treatment of those infected Education, treatment, counseling for partners of infected individuals Education and Counseling of At risk persons Pre-exposure vaccination of individuals at risk for vaccine- preventable disease CDC STD TG 2010
Interactive Counseling Basics Partners: past 2 months, 12 months, m/f/both? Prevention of Pregnancy: How are you preventing pregnancy? Protection from STDs: What do you use to protect from STD and HIV? Practices: What kind of sex; safe? Past History of STDs: You? Any of your partners? CDC STD TG 2010
Physical and Chemical Barriers • Proper use yields benefit! (structural failure 2%) • Female condoms are available but relatively more expensive than male condoms (PE or Nitrile), relatively few studies, recommended. • Chemical barriers have long been used as spermicides (OTC N9) • Spermicides gave birth to a decade of research on chemical barriers to STDs www.cdc.gov/condomeffectiveness/latex.htm
Prevention via microbicide • N9 (surfactant) irritant, not recommended • Buffer gel (pH control), not effective so far • Carraguard ( HIV entry inhibitor), not effective • Cellulose sulfate (entry inhibitor), not effective • SAVVY (surfactant), not effective • Pro2000 (polyanion), not effective • Hopeless? www.microbicide.org
Microbicide Promise • Study in South Africa (CAPRISA) • Tenofovir Gel (Reverse Transcriptase Inhibitor) • Double Blind, Placebo Controlled, Randomized Prevention Trial • 18-30 y.o. / 30 month study (660-680 women- years) • 39% overall reduction in HIV (54% in high adherence participants) Karim et al. Science 329: 1168 (September 2010)
Research Continues… • HIV is the major goal (other STDs also targeted) • HIV focuses on NRTI, NNRTI, fusion inhibitors • HSV is also on the radar • Multivalent prevention is of interest but broad spectrum compounds did not succeed • Delivery is important not just vaginal gel • Vaginal rings, 30 day efficacy, coital independence • Vaccine?
Vaccine Preventable Disease • Molecular biology is bringing new potential vaccines into the pipeline • Molecules that bind pathogen to host cell, factors that are essential to pathogenesis, common antigens for all strains of a pathogen can be identified and cloned • Cloned antigens can be used to produce monoclonal antibodies, antibody fragments, or immunizing carriers for STDs • But, molecular biology can move faster than product development and testing • Conserved antigens and mutation rate a key
Knowing People Knowing Place Populations
Who needs special attention? • Pregnant women • Adolescents • Children • Persons in correctional facilities • MSM • WSW
Pregnancy Issues • Screening • For what (HIV, TP, HBV, CT, GC, HCV) • When to screen first, when to repeat • Concerns • Perinatal infections, preterm birth • Transplacental drugs • Vaccinations for mother and newborn • Referral • Circumstances requiring referral
Pregnancy Recommendations 2010 (Screening) Do not screen BV or Trich (unless symptomatic) or HSV-2 unless previously diagnosed
The final common pathway to parturition • Pathogen engages TLR • Signal transduction leads to cytokine and chemokine production • Cytokines recruit inflammatory cells which provide matrix metalloproteinases (membranes, cervical remodeling) • Cytokines induce COX, PG, NOS (cervical ripening and uterine contractions) Preterm Birth. IOM. National Academies Press 2007
Adolescent Issues • Early initiation of sex -> risk • Parental consent not required for STD services • Biological susceptibility may be greater • Unfamiliar with obtaining medical care • Protecting confidentiality (EOB mailed to parents) • Screening (for CT, GC, HIV, CxCa) • Prevention (HPV, Education and Counseling)
STD and Children • GC, CT, TP acquired in the neonatal period is a virtual guarantee of sexual contact • HPV and vaginitis are not definitely indicative of sexual contact • Investigation involves clinicians, laboratorians, child protection officials • Time is of the essence
Issues of Incarcerated Individuals • High rates of STD (especially Juvi) • Concentrated correlates of risk • Low SES • Urban centered • Racial minority • Commercial or coerced sex • History of poor or no medical care • Protocols for care are not uniform • Funding for facilities and STD services uncertain
MSM Issues • Shifting landscape in recent past • HIV infected persons living longer and healthier • Substance abuse patterns changing • Demographic shifts in MSM populations • Partner networking via social media • Actual practices (ie oral sex) influence which organisms are spread (not HIV, but other STIs) • Specific risks must be assessed on an individual basis • Diagnostic testing (HIV, CT, GC, TP, HSV2, HBsAg, anal cytology) • Vaccination (HAV, HBV)
WSW Issues • Do not assume WSW are not at risk • Risks are linked to specific behaviors • Research data is limited by sexual transmission of HSV2, TV, BV have been reported • Some WSW also have had sex with men, or are having sex with men CDC STD TG 2010
Particular Recommendations
GC and CT (2009 Summary) USA 99.1 (20.5 th) GC 7.2 / 100 K 107.2 / 100 K (19th) 246.2 / 100 K 159.7 / 100 K 340.8 / 100 K (34th) 802.7 / 100 K CT USA 409 (20.5 th) CDC STD Surveillance 2009
GC and Antibiotics • Recommendation CTX + AZITH or DOX • Dual coverage (CT/GC) advocated for either • CTX dosage recommended doubled since 2007 • GISP noted creeping MICs for urethral GC • MIC creep is a harbinger of resistance • % R in past 10 years: 0.2% -> 1.4% for Cefixime • % R in past 10 years: 0.1% -> 0.3% for Ceftriaxone • Cephalosporin resistance from Asia and minimally HI (travel history may influence therapy)
GC and Azithromycin • AZITH not primary drug for GC, but exposure to drug may select for resistance • Mutation of mtrR releases GC from repression of drug efflux pump (stuck in on position) • Genetic transfer of mtrR mutation to wild type bacterium increases AZITH resistance 10 fold (lab) • Now known that mtrR regulates 70 genes • 23s rRNA mutation blocks macrolide binding site on 50s bacterial ribosome [C2599T or A2143G] • In 2010, 22% of 149 GC isolates in one month were ERY/AZITH resistant Zarantonelli 1999 AAC 43:2468 / Galarza 2010 AAC 54: 1652
The power of 2 • CT and GC are simultaneously treated because of similar epidemiology and sequelae • Two antibiotics have an advantage for preventing resistance development • Hypothetical: Development of resistance to antibiotic A occurs 1 in 1 million bacteria; resistance to antibiotic B occurs 1 in one million bacteria. The chance of simultaneous resistance is 1 x 10-12 • Transferrable resistance is a different matter
Azithromycin for Chlamydia • AZTH named before DOX in recommendations • Single 1g dose AZTH vs 7days DOX (100 mg BID) • Meta analysis of 12 RCT • AZTH 97% and DOX 98% microbiologic cure rate • Clinically equivalent for genital tract infection • AZTH supports DOT therapy when multi-dosing is uncertain • Regardless of AZTH or DOX, abstinence for 7 days is recommended Lau et al. Sex. Transm. Dis. 2002; 29: 479
Mycoplasma genitaliumUrethritis and Cervicitis • GC and CT most common, but NGU may involve MG 15-25% of the time, but no standardized MG test • Other mycoplasmas and Ureaplasma are inconsistent as etiologies • Cervix, like urethra, shows pus or muco pus • GC and CT may be found, but most often no organism cultured • MG has been implicated in cervicitis (also HSV,Trich,BV). • Treatment is single dose AZTH CDC STDTG 2010
Expanded diagnostic guidelines for Trichomonasvaginaliscervicitis • Cervicitis may imply upper tract inflammation; look for PID signs • Along with GC/CT(NAAT) evaluate for BV and TV • Microscopy is <50% sensitive for TV • If microscopy is negative use TV culture or FDA cleared method (OSOM, Affirm) • Alternate to metronidazole is tinidazole • CDC recommends treatment of BV or TV CDC STDTG 2010
Syphilis and HIV (2009 Summary) USA 4.6 (13.5 th) Syphilis 0 / 100 K 2.5 / 100 K (26th) 16.8 / 100 K 2.3 / 100 K 8.3 / 100 K 33 / 100 K HIV (estimates) USA 17.4 CDC STD Surveillance 2009
Azithromycin and syphilis • Guidelines emphasize that syphilis remains susceptible to penicillin which is the recommended treatment • Desensitization is recommended for allergy • AZTH has been used as an alternative • A SNP in the rRNA gene of the 23S ribosome inactivates the macrolide binding site in TP • Concern probably mostly theoretical now Katz and Klausner. CurrOpin I D. 2008; 21: 83
Neuro-Syphilis (NS) and CSF • HIV with Syphilis has significant implications for NS (HIV causes CSF pleiocytosis and risk for NS) • Syphilis: common comorbidity w/HIV (MSM especially) • NS may occur early in the infection (not just tertiary) • Older recommendations conservative regarding LP • Experts are moving toward universal LP for HIV with syphilis (CSF VDRL: specific but insensitive) • NS treatment is more aggressive than early syphilis alone CDC STDTG 2010
New NS Biomarkers • With HIV, a >20 WBC/uL increases specificity for NS diagnosis • CSF FTA-Abs is less specific than VDRL but more sensitive (with Neg FTA, NS unlikely) • Marra discovered that CXCL 13 elevated in CSF and serum of NS but not in HIV (OR 2.23 / log titer) and declines after NS treatment • CXCL 13 test is independent of CSF WBC, plasma HIV RNA, peripheral CD4+ and RV meds Marra et al. STD 2010; 37:283
Bacterial Vaginosis • Not really an infection but dysbiosis (often asymptomatic) • Diagnosis by Gram Stain smear or Amsel Criteria • Concern relates to risk associations • HIV, GC, CT, HSV2 • Premature birth, postop infections • PID • Treatment is oral Metronidazole or topical metronidazole or clindamycin • Alternative is Tinidazole CDC STD TG 2010
Genital Warts • Approach may be patient administered or provider administered • In addition to Podofilox or Imoquomid, patient may use Sinecatechins • Provider may administer cryotherapy, podophyllin resin, TCA or BCA, surgical excision
Concluding Thoughts… • STD is not the sole domain of public health officials • Medical history taking and health counseling provides opportunity to impact STD • Updated opinions on best practices are routinely update by the CDC • “Putting our mouth where our money is” will emphasize viral rather than bacterial STD • While 11 new topics did not emphasize virus attention to HIV and HPV still need to remain elements of concern