Download
1 / 1
10 likes | 304 Vues
RA. OA. Variable. (N=15,784). (N=3,639). Variable. HR. 95% CI. p. Age in years (mean ± SD). 62 ± 13. 67 ± 12. Age. 1.05. 1.04-1.06. 0.001. Disease Duration in years (mean ± SD). 15 ± 11 . 17 ± 11. Caucasian . 4.12. 1.95-8.71. 0.001. Proportion Male (%). 23. 17.

E N D
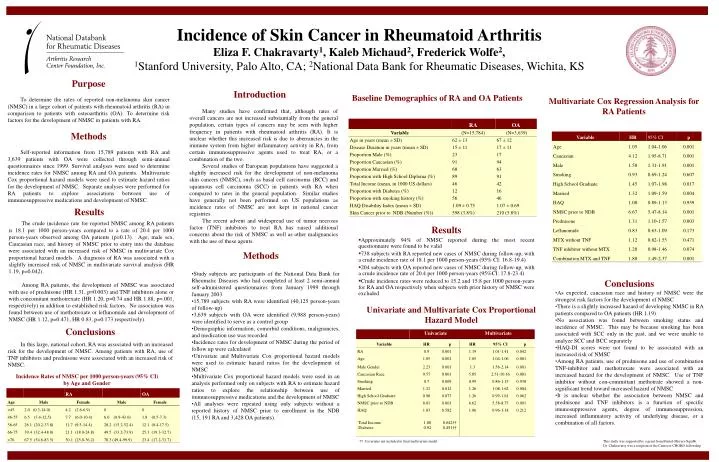
RA OA Variable (N=15,784) (N=3,639) Variable HR 95% CI p Age in years (mean ± SD) 62 ± 13 67 ± 12 Age 1.05 1.04-1.06 0.001 Disease Duration in years (mean ± SD) 15 ± 11 17 ± 11 Caucasian 4.12 1.95-8.71 0.001 Proportion Male (%) 23 17 Proportion Caucasian (%) 91 94 Male 1.58 1.31-1.91 0.001 Proportion Married (%) 68 63 Smoking 0.93 0.69-1.24 0.607 Proportion with High School Diploma (%) 89 91 High School Graduate 1.45 1.07-1.98 0.017 Total Income (mean, in 1000 US dollars) 46 42 Proportion with Diabetes (%) 12 16 Married 1.32 1.09-1.59 0.004 Proportion with smoking history (%) 56 46 HAQ 1.00 0.89-1.13 0.959 HAQ Disability Index (mean ± SD) 1.09 ± 0.75 1.07 ± 0.69 NMSC prior to NDB 6.67 5.47-8.14 0.001 Skin Cancer prior to NDB (Number (%)) 598 (3.8%) 210 (5.8%) Prednisone 1.31 1.10-1.57 0.003 Leflunomide 0.83 0.63-1.09 0.173 MTX without TNF 1.12 0.82-1.55 0.471 TNF inhibitor without MTX 1.20 0.98-1.46 0.074 Combination MTX and TNF 1.88 1.49-2.37 0.001 Variable HR p HR 95% CI p RA 0.9 0.001 1.19 1.01-1.41 0.042 Age 1.05 0.001 1.05 1.04-1.06 0.001 Male Gender 2.23 0.001 1.3 1.56-2.14 0.001 Caucasian Race 9.57 0.001 5.05 2.51-10.16 0.001 Smoking 0.7 0.009 0.99 0.86-1.15 0.938 Married 1.21 0.012 1.26 1.08-1.62 0.004 RA OA High School Graduate 0.98 0.873 1.26 0.99-1.61 0.062 Age Male Female Male Female NMSC prior to NDB 8.01 0.001 6.62 5.58-8.75 0.001 <45 2.0 (0.3-14.0) 4.2 (2.6-6.9) 0 0 HAQ 1.03 0.582 1.06 0.96-1.18 0.212 46-55 6.5 (3.4-12.5) 7.7 (6.0-10.4) 6.0 (0.9-43.0) 1.8 (0.5-7.3) 56-65 26.1 (20.2-33.8) 11.7 (9.5-14.4) 28.2 (15.2-52.4) 12.1 (8.4-17.5) 66-75 39.4 (32.4-48.0) 21.1 (18.0-24.8) 49.5 (33.2-73.9) 25.1 (19.3-32.7) >76 67.5 (54.6-83.5) 30.1 (25.0-36.2) 70.3 (49.4-99.9) 23.4 (17.2-31.7) Incidence of Skin Cancer in Rheumatoid Arthritis Eliza F. Chakravarty1, Kaleb Michaud2, Frederick Wolfe2, 1Stanford University, Palo Alto, CA; 2National Data Bank for Rheumatic Diseases, Wichita, KS Purpose To determine the rates of reported non-melanoma skin cancer (NMSC) in a large cohort of patients with rheumatoid arthritis (RA) in comparison to patients with osteoarthritis (OA). To determine risk factors for the development of NMSC in patients with RA. Methods Self-reported information from 15,789 patients with RA and 3,639 patients with OA were collected through semi-annual questionnaires since 1999. Survival analyses were used to determine incidence rates for NMSC among RA and OA patients. Multivariate Cox proportional hazard models were used to estimate hazard ratios for the development of NMSC. Separate analyses were performed for RA patients to explore associations between use of immunosuppressive medications and development of NMSC. Introduction Baseline Demographics of RA and OA Patients Multivariate Cox Regression Analysis for RA Patients Many studies have confirmed that, although rates of overall cancers are not increased substantially from the general population, certain types of cancers may be seen with higher frequency in patients with rheumatoid arthritis (RA). It is unclear whether this increased risk is due to aberrancies in the immune system from higher inflammatory activity in RA, from certain immunosuppressive agents used to treat RA, or a combination of the two. Several studies of European populations have suggested a slightly increased risk for the development of non-melanoma skin cancers (NMSC), such as basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) in patients with RA when compared to rates in the general population. Similar studies have generally not been performed on US populations as incidence rates of NMSC are not kept in national cancer registries. The recent advent and widespread use of tumor necrosis factor (TNF) inhibitors to treat RA has raised additional concerns about the risk of NMSC as well as other malignancies with the use of these agents. Results The crude incidence rate for reported NMSC among RA patients is 18.1 per 1000 person-years compared to a rate of 20.4 per 1000 person-years observed among OA patients (p=0.13). Age, male sex, Caucasian race, and history of NMSC prior to entry into the database were associated with an increased risk of NMSC in multivariate Cox proportional hazard models. A diagnosis of RA was associated with a slightly increased risk of NMSC in multivariate survival analysis (HR 1.19, p=0.042). Among RA patients, the development of NMSC was associated with use of prednisone (HR 1.31, p=0.003) and TNF inhibitors alone or with concomitant methotrexate (HR 1.20, p=0.74 and HR 1.88, p=.001, respectively) in addition to established risk factors. No association was found between use of methotrexate or leflunomide and development of NMSC (HR 1.12, p=0.471, HR 0.83, p=0.173 respectively). Results • Approximately 94% of NMSC reported during the most recent questionnaire were found to be valid • 738 subjects with RA reported new cases of NMSC during follow-up, with a crude incidence rate of 18.1 per 1000 person-years (95% CI: 16.8-19.4) • 204 subjects with OA reported new cases of NMSC during follow-up, with a crude incidence rate of 20.4 per 1000 person-years (95%CI: 17.8-23.4) • Crude incidence rates were reduced to 15.2 and 15.8 per 1000 person-years for RA and OA respectively when subjects with prior history of NMSC were excluded Methods • Study subjects are participants of the National Data Bank for Rheumatic Diseases who had completed at least 2 semi-annual self-administered questionnaires from January 1999 through January 2003. • 15,789 subjects with RA were identified (40,125 person-years of follow-up) • 3,639 subjects with OA were identified (9,988 person-years) were identified to serve as a control group • Demographic information, comorbid conditions, malignancies, and medication use was recorded • Incidence rates for development of NMSC during the period of follow up were calculated • Univariate and Multivariate Cox proportional hazard models were used to estimate hazard ratios for the development of NMSC • Multivariate Cox proportional hazard models were used in an analysis performed only on subjects with RA to estimate hazard ratios to explore the relationship between use of immunosuppressive medications and the development of NMSC • All analyses were repeated using only subjects without a reported history of NMSC prior to enrollment in the NDB (15, 191 RA and 3,428 OA patients). • Conclusions • As expected, caucasian race and history of NMSC were the strongest risk factors for the development of NMSC • There is a slightly increased hazard of developing NMSC in RA patients compared to OA patients (HR 1.19) • No association was found between smoking status and incidence of NMSC. This may be because smoking has been associated with SCC only in the past, and we were unable to analyze SCC and BCC separately • HAQ-DI scores were not found to be associated with an increased risk of NMSC • Among RA patients, use of prednisone and use of combination TNF-inhibitor and methotrexate were associated with an increased hazard for the development of NMSC. Use of TNF inhibitor without con-committant methotrate showed a non-significant trend toward increased hazard of NMSC • It is unclear whether the association between NMSC and prednisone and TNF inhibitors is a function of specific imunosuppressive agents, degree of immunosuppression, increased inflammatory activity of underlying disease, or a combination of all factors. Univariate and Multivariate Cox Proportional Hazard Model Conclusions In this large, national cohort, RA was associated with an increased risk for the development of NMSC. Among patients with RA, use of TNF inhibitors and prednisone were associated with an increased risk of NMSC. Incidence Rates of NMSC per 1000 person-years (95% CI) by Age and Gender Total Income 1.00 0.842†† Diabetes 0.92 0.451†† †† Covariates not included in final multivariate model This study was supported by a grant from Bristol-Meyers-Squibb. Dr. Chakravarty was a recipient of the Centocor CHORD fellowship