Download
1 / 33
340 likes | 523 Vues
Sickle Cell Trait in Athletes. Jason Blackham MD CAQSM Clinical Assistant Professor Internal Medicine And UI Sports Medicine Center. Introduction. Cases History Pathophysiology Complications Screening Symptoms Cautions What to do about it?. Case #1.

E N D
Sickle Cell Trait in Athletes Jason Blackham MD CAQSM Clinical Assistant Professor Internal Medicine And UI Sports Medicine Center
Introduction • Cases • History • Pathophysiology • Complications • Screening • Symptoms • Cautions • What to do about it?
Case #1 • 19 yo healthy African American Div I freshman DE during preseason conditioning • Atraumatic, painless tea to bright red urine • Cramping in paraspinal muscles • No recent heat illness, dysuria, polyuria, fever, myalgias, sore throat, rashes, trauma, or previous episodes. • Used whey protein shake daily. • MEDs: Occasional ibuprofen, none in past 7 days • FHx: Sister with sickle cell disease
Case #1 Exam • VS: 97.7°F, 18, 72, 130/75, 242 lbs • GEN: Healthy, NAD • ABD: BS normoactive, soft, NT, ND, no HSM, no CVAT • GU: Male genitalia normal without lesions, discharge, or testicular mass • SKIN: No rashes, petechiae, skin lesions • EXT: No edema
Case #1 LABS • UA - SG 1.020, 1+ prot, 4+ heme, LE + • Micro - RBC TNTC with dysmorphia • Urine Culture - Negative • Normal CBC, CMP, CK, PT, PTT, INR
Case #1 LABS • No exercise or lifting for one week • UA - SG 1.015, 1+ prot, 4+ heme, LE + • Micro - RBC TNTC, no dysmorphia • Heme Electrophoresis - Sickle cell trait • Normal abdomen/pelvis CT • Referred to urology • Cystoscopy - bleeding from L kidney
Case #1 Treatment • Epsilon aminocaproic acid and Na bicarb for 2 weeks • UA - SG 1.010, no prot, heme, LE, RBC • Morning urine - SG 1.020 • Gradually transitioned back to conditioning without recurrence
Case #2 • 16 yo African American high school football player in North Carolina • Summer football practice without pads • 1 hr • Severe Cramps • ? of mental status changes • Fell in exhaustion. • EMS took to ER.
Case #2 LABS • Rectal temp 36.3 Pulse 109 • PE unremarkable • WBC 15.4 • Cr 1.3 0.7 • AST 1320, ALT 465 • CK 138,120 8,936 • UA- trace protein, 3+ blood, no RBC. • Sickle cell trait • 5L NS IV in ED. • Admitted to ICU for • Heat exhaustion • Rhabdomyolysis
Case #2 • Next year • After returning from knee arthroscopy • Conditioning at football practice • Dizziness, weakness, mental status changes • Cramping, ? of syncope • Cr 1.4, CK 489, UA SG 1.010, trace Prot. • EMS took to ER • Felt better after 1L NS.
Case #2 Treatment • Calculated sweat loss to recommend appropriate fluid intake • Recommended guidelines for exercise limitations • Returned to play gradually and finished season his senior year
Sickle Cell Trait • History • Pathophysiology • Complications • Screening • Symptoms • Cautions
Sickle Cell Trait History • 1970 Four Deaths in Military Recruits • 4 more with exertional rhabdomyolsis • 1974 Colorado football player died • 1970-1985 Several collapses and deaths in military. • Air Force temporarily banned SCT applicants
Deaths - SCT • Sudden death in athletes • 1- Cardiovascular • 2- Heat illness • 3- Rhabdomylosis with SCT • 4- Asthma Med Sci Sports Exer 1995;27(5):641-647 Arch Intern Med 1996 156(20):2297-2302
Deaths – Military data • 1987 • RR 28 compared with black recruits CI 11-84 • RR 40 compared with all recruits • Rate 1/3200 per training cycle • 1994 • RR 21 compared with black recruits CI 10-43 • Rate 1/5,500 per training cycle NEJM1987;317(13):781-7 Semin Hematol 1994;31(3):181-225
College Football Deaths with SCT Eichner GSSI #103, 2006;19(4)
College Football Deaths • 2006-2007 • Rice, after running • University of Southern Florida • Deaths from exertional rhabdomyolysis or cardiac death from arrhythmia
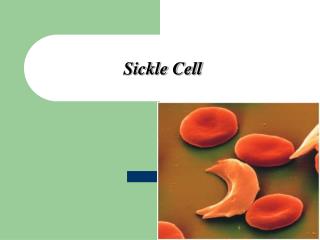
Pathophysiology • Point mutation on Beta-chain of hemoglobin • Homozygous • Sickle cell disease • Conformational change + sickling • Heterozygous • Sickle cell trait • Normally benign
Pathophysiology • In the kidney medulla • Hyperosmolar • Hypoxic – anaerobic • Acidotic • Sickling in vasa recta leading to obstruction • Microscopic infarction of medulla • Papillary necrosis • Rupture of arterioles NEJM 1985;312(25):1623-31 J Am Soc Nephrol 1997;8:1034-40 Am J Hematol 2000;63:205-11
But with exercise • Lactic acidosis especially muscle capillaries • Elevated body temperature • Hyperosmolar drives fluid out of RBC • Increases concentration of hemoglobin S • Hypoxia in muscle • Leads to sickling, necrosis, rhabdomyolysis Phys Sportsmed 1990;18(11):53-63 Phys Sportsmed 1993;21(7):51-64
Risk factors for sickling • Altitude • Heat stress • Rapid conditioning • Sustained maximal exertion Phys Sportsmed 1993;21(7):51-64
Complications • Hematuria • Inability to concentrate urine • Glaucoma- bleeding in anterior chamber • Splenic infarction • Cramps • Exertional rhabdomyolysis • Increased risk of heat illness • Sudden collapse Phys Sportsmed 1993;21(7):51-64 Sem Hematology 1994;31(3):181-225
Renal • Hematuria • 2.5% of hospitalized Vets, RR 1.98 • Expert opinion, 3-4% • 80% from LEFT kidney • Epidemiology in athletes and effect of exercise is not known • Papillary necrosis • Infarctions in medulla • Inability to concentrate urine • Disrupted countercurrent exchange in medulla • Progresses with age and may lead to dehydration NEJM 1979;300(18):1001-5 NEJM 1985;312(25):1623-31 J Am Soc Nephrol 1997;8:1034-40
Spleen • RBC’s sickle in hypoxic environment • Removed in spleen • “Plug up” vessels in spleen • Thrombosis leads to splenic infarction • Most cases are at altitude >7000 ft Semin Hematol 1994;31(3):181-225
Spleen • LUQ severe pain • n/v • Splinting, left pleural effusion and atelectasis • Palpable spleen • Fever • Elevated WBC • LDH elevated higher than CK, AST, ALT • Usually self limited not requiring surgery
Muscle • Rhabdomyolysis • Necrosis
Screening • Recommendations to screen for SCT • 6-14%, average 8% of African Americans • Is it preventable?
Presentation • Ischemic pain in low back, buttock and leg muscles with weakness • “Cramps” • Sudden without warning • Muscles give out and look normal • Occurs early in season and training sessions • Normal body temperature • With oxygen, fluids, cold tub • Feel fine in 10-15 minutes • Can talk when collapse
Precautions for SCT athletes • Acclimatize gradually • Monitor hydration • Avoid diuretics • Consider testing urine concentrating ability in first AM void • Modify workouts, condition gradually • Avoid sprints or repeats over 500m, and timed runs over ½ mile Semin Hematol 1994;31(3):181-225 Phys Sportsmed 1993;21(7):51-64 NCAA Sports Medicine Handbook 2006-7, pg 74-5 GSSI #103, 2006;19(4)
Precautions for SCT athletes • No participation during illness • Avoid or acclimatize to altitude • If cramping, heat illness or unusual symptoms • IV fluids, supplemental O2, cooling • If doesn’t improve, transport to ED Semin Hematol 1994;31(3):181-225 Phys Sportsmed 1993;21(7):51-64 NCAA Sports Medicine Handbook 2006-7, pg 74-5 GSSI #103, 2006;19(4)
Precautions and Screening • Does it help? • No prospective data in sports • After military implemented protocols, number of cases reduced • 1982-1986 compared with 1977-1981 • RR dropped to 11 • Rate dropped from 32 to 14 per 100,000 Semin Hematol 1994;31(3):181-225
Key Points • 3rd cause of death in athletes • Distinguish from heat cramps • Complications • Hematuria, splenic infarction, rhabdomyolysis • May be preventable
References • Eichner. Phys Sportsmed 1990;18(11):53-63 • Jones et al. Clin J Sport Med 1997;7(2)119-25 • Heller, et al. NEJM 1979;300(18):1001-5 • Scully, et al. NEJM 1985;312(25):1623-31 • Diggs. Aviat Space Environ Med 1984;55(5):358-64 • Zadeii, et al. J Am Soc Nephrol 1997;8:1034-40 • Kark et al. Semin Hematol 1994;31(3):181-225 • Kark et al. NEJM 1987;317(13):781-7 • Ataga et al. Am J Hematol 2000;63:205-11 • Warren et al. Pediatrics 1999;103(2):22-4 • Eichner. Phys Sportsmed 1993;21(7):51-64 • Eichner Gatorade Sports Science Institute, Sports Science Exchange 103, 2006;19(4):1-6 • NCAA Sports Medicine Handbook 2006-7, pg 74-5 • Van Camp et al. Med Sci Sports Exer 1995;27(5):641-647 • Thompson et al. Arch Intern Med 1996; 156(20):2297-2302