Download
1 / 40
400 likes | 813 Vues
What’s All the Fuss About Clostridium difficile ?. Peter C. Iwen, PhD, D(ABMM) Nebraska Public Health Laboratory. Clostridium difficile – GI Disease. Indigenous microflora of colon 1 trillion bacteria per gram!. Objectives. C. difficile ….the organism Host relationships and pathogenesis

E N D
What’s All the Fuss About Clostridium difficile? Peter C. Iwen, PhD, D(ABMM) Nebraska Public Health Laboratory
Clostridium difficile – GI Disease Indigenous microflora of colon 1 trillion bacteria per gram!
Objectives • C. difficile ….the organism • Host relationships and pathogenesis • Diagnosis • Prevention and control • Patient management • Update clinical issues
National Estimates of US Short-Stay Hospital Discharges with C. difficile as First-Listed or Any Diagnosis From McDonald LC, et al. Emerg Infect Dis. 2006;12(3):409-15
Clostridium difficile • Bacterium • Anaerobe • Gram-positive spore-forming bacillus • Source • Environment • Stool flora
Host Relationship Disturbed colonic microflora ↓ C. difficile exposure & colonize ↓ Toxin A & B ↓ Diarrhea & colitis
Risk Factors • Age >65 years • Severe underlying disease • Prompting hospitalization • Nasogastric intubation • Antiulcer medications • Proton pump inhibitors • Antimicrobial therapy • Clindamycin, 3rd generation cephalosporins, penicillin, fluoroquinolones • Long hospital stay or long-term care residency “Clostridium difficile is the most common cause of nosocomial infectious diarrhea.”
Sunenshine and McDonald, Cleveland Clin. J. Med., Feb 2006
Virulence Factors • Toxin A • Exotoxin • Enterotoxic to cells • Toxin B • Exotoxin • Not as toxic to cells? • Multiple strains of C. difficile • ToxA+/ToxB+ • ToxA+/ToxB- • ToxA-/ToxB+ …only toxigenic strains of C. difficile produce disease…
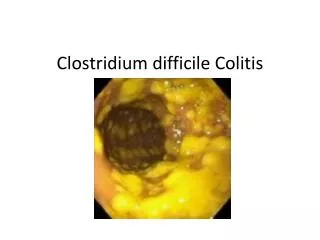
Clinical Presentation • Mild disease • Non-bloody diarrhea • Mild abdominal tenderness • Severe disease • Pseudomembranous colitis • Paralytic ileus • Ileitis • Toxic megacolon • Ulcerative colitis • Perforation • Ascites
Pseudomembranous Colitis Yellow lesion against hyperemic bowel Mushroom-shaped pseudomembrane→ “Volcano” lesion H & E, OM 400x
Diagnostics • Generally…. …if stool samples are obtained after hospital day 3, the only enteric pathogen most labs will test for is…..Clostridium difficile….. • Testing not considered a STAT test • Batching, but calling all positive results • Many labs will only test a diarrheic stool specimen • Follow-up testing of previous positive result not useful • Patients remain positive for months • Not useful for “proof-of-cure”
Relative Sensitivity Culture > Cell cytotoxin > Toxin A & B EIA > Toxin A EIA > Latex agglutination > Endoscopy
What about PCR? • Studies have shown PCR to be less sensitive than the toxin assay • Requires a nucleic acid extraction step • Complexity of stool matrix a problem
CDI Case Defined • Stool characteristic • Diarrhea (most common) • No diarrhea • Associated with toxic megacolon or ileitis • Documented by radiology • ≥ 1 of the following • Stool positive for: • C. difficile toxin • C. difficile determined to be a toxin producer • Pseudomembranous colitis by: • Endoscopy • Histological exam
Prevention and Control • Prevent ingestion of the organism • Infection control strategies • Target environment • Personal hygiene • Barrier methods • Reduce the chance of disease in the event of such digestion • Minimize or eliminate antibiotic exposure • “Good antimicrobial stewardship”
Audience Interaction • Clostridium difficile spores can resist desiccation and can persist on hard surfaces: • 48 hours or less • About 1 week • About 1 month • > 6 months
The most effective cleaning agent for killing C. difficile spores in the environment is: A. 70% alcohol B. 10% bleach C. Hot water and soap D. Phenol solutions E. Quaternary ammonium compounds Enhanced environmental cleaning…sporocidal
The incubation period for Clostridium difficile infection is: • Less than 1 day • 1-7 days • 2-3 weeks • Unknown
Barrier precautions to prevent the spread of Clostridium difficile include: • Airborne precautions • Droplet precautions • Contact precautions • Standard precautions only Single room Gloves Gowns Duration of isolation controversial …2 days after diarrhea resolves …upon discharge
Patient Management Surgical consult…perforation, toxic megacolon, colonic-wall thickening, ascites….
“Stool infusion therapy” or “fecal transplant” has been shown to be highly effective….
Update Clinical Issues • Hypervirulent C. difficile strain • Community-associated CDI • Proton Pump Inhibitors as risk factor • Antacids and antiulcer drugs • Medicare issues and CDI
Hypervirulent C. difficile Strain • North American PFGE Type 1 • Restriction enzyme analysis Type BI • PCR ribotype 027 Collectively referred to as “NAP1/BI/027 strain”
NAP1 Virulence Attributes • Hypertoxigenic • Toxin A 16x • Toxin B 23x • Binary toxin • Hypersporulation capacity • High-level resistance to fluoroquinolones • Leads to outbreaks
States with the Epidemic Strain of C. difficile Confirmed by CDC and Hines VA labs (N=24),Updated 2/9/2007 DC HI PR AK
Community-Acquired CDI • Less common than nosocomial • No traditional risk factors • “Spontaneous” • Exposure to hypervirulent strain • More likely to receive antacids (anti-ulcer) drugs
Heartburn Drugs Cause Diarrhea? • Proton pump inhibitors • Prilosec • Prevacid • Nexium • H2 blockers • Zantac • Pepcid • Tagamet • Main function is to suppress stomach acid production • Gastritis • GERD (acid reflux disease) • Heartburn S. Dial, 2005, J. Amer. Med Assoc., 293:2989-2995.
Stomach Acid-Suppressing Medications and Community-Acquired CDAD, England From Dial S, et al. JAMA. 2005;294:2989-2995.
Deficit Reduction Act of 2005 • Requires an adjustment in Medicare Diagnosis Related Group payments • For certain hospital-acquired conditions
“Myth Busters” • C. difficile may infect individuals who are NOT taking antibiotics • Optimal method to diagnose CDI is NOT clear • Alcohol-based gels are NOT effective for hand hygiene against C. difficile spores • Vancomycin is NOT the recommended initial therapy for CDI • Current literature does NOT support the use of probiotics to treat for CDI • CDI is NOT only a problem in acute care hospital facilities but also long-term care and rehab centers
Recommendations for Control • Conduct surveillance for CDI • Early diagnosis and treatment • Strict infection control practices • Good antimicrobial stewardship
Clostridium difficile Infection Questions??