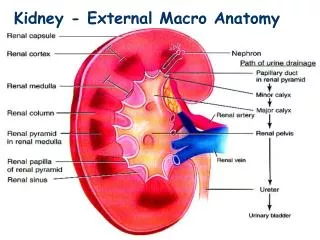
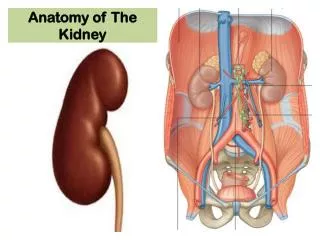
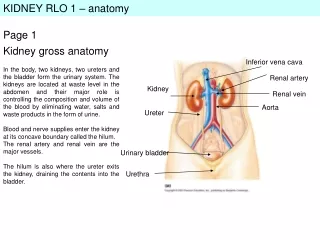
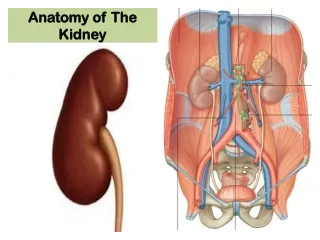
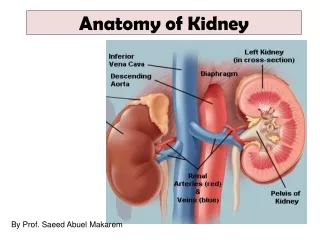
Anatomy-Kidney
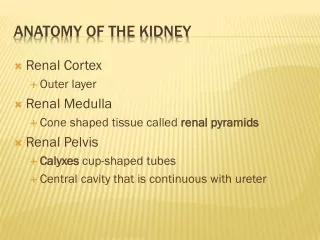
Anatomy-Kidney. Congenital Anomalies:. Agenesis Fusion Dysplasia Simple cysts Polycystic kidney disease. Urolithiasis – Stones:. Urolithiasis – stones:. Infection. Calcium Stone-Formation. Infected Stone-Formation. Urinary NH 4 +. CaP supersaturation. Urinary pH.

Anatomy-Kidney
E N D
Presentation Transcript
Congenital Anomalies: Agenesis Fusion Dysplasia Simple cysts Polycystic kidney disease
Urolithiasis – stones: Infection
Infected Stone-Formation Urinary NH4+ CaP supersaturation Urinary pH Urinary tract infection with a urea- splitting organism Nucleation and agglomeration Urinary mucoprotein Abnormal crystalluria Infection stone Urinary citrate Inhibitory activity Urinary phosphate
Uric Acid Stone-Formation Age Sex (M > F) Genetic disorders Metabolic disorders Dietary purine Urinary uric acid Renal NH3 production Dietary acid Uric acid stone Urinary pH Uric acid supersaturation Abnormal crystalluria Urinary volume Fluid intake Fluid loss Ambient temperature
Cystine Stone-Formation Tubular reabsorption of cystine Cystine supersaturation Abnormal crystalluria Cystine stone Urinary cystine Possible metabolic factors
Clinical picture of stone • Depend on the site • Asymptomatic • Pain:( kidney dull ach – ureterureteric colic -bladder suprapupic pain reffered to the tip of pines – urethral ) • Symptoms of complication • Hematuria • Infection • Migration • Obstruction • Malignancy
Diagnostic evaluation for stone • History, P/E • Urine • PH>7.5 Infected stones • PH<5.5 Uric acid • Sediment for crystalluria • Urine culture –urea splitting organisms • Biochemical screen • U&E, Ca,PO4, uric acid, bicarbonate • PTH if Ca is elevated • Radiological (plain x ray – IVU- ascending urogram-CT) • US • Stone analysis
Treatment I)For acute attack: analgesics and II)Definitive treatment • Conservative : <1cm with no complication and no distal obstruction ( fluid ,antispasmodics, change urine PH, antibiotics & follow up ) B)Active (ESWL-Percutanousenephro- lithotomy, nephro- lithotomy ,Pyelo-lithotomy,Retrograde endoscopy, uretrolithotomy ) III)Treatment of complication( calculasanuria, hydronephrosis and pyonephrosis) IV)Prevention of recurrence etiology Multiple : urethral –ureter-kidney-bladder
Renal tumors • Benign (rare!) • Adenoma, oncocytoma, angiomyolipoma, fibroma • Malignant: • Renal cell carcinoma (common – adults) • Wilm`stumor (childhood) • Transitional cell carcinoma of renal pelvis
Wilm’s Tumor Nephroblastoma. Synonyms: Most common renal tumor of childhood. Peak age - 2.5 - 3.5 years. Incidence: Etiology: Embryonic renal tissue (metanephric blastema). Genetic abnormalities. Clinical Features: radiology Palpable abdominal mass. Abdominal pain, fever, anorexia, nausea/vomiting. CT ,us No specific clinical laboratory findings. Diagnosis by radiographic techniques. Path: Gross: Solitary/multiple cystic mass, sharply delineated. Soft, bulging, gray-white with focal hemorrhage and necrosis. Course: 5-yr. Survival 80%. Metastases to lung, liver, bone, brain. Treatment: Resection with chemotherapy ± radiotherapy.
Renal Cell Carcinoma: Hypernephroma, clear cell carcinoma. Synonyms: 5th and 6th decades, most common primary renal malignancy. Incidence: Etiology: Cells of proximal convoluted tubule. Risk factors are smoking, obesity, analgesic abuse Clinical Features: Hematuria*, flank pain, palpable mass. Frequently metastasize (lungs, bone, skin, liver, brain). Lab: Gross or microscopic hematuria. CT Renal mass Clinical Course: 5-yr. survival 40%. Poor prognosis with metastases. Treatment: Chemotherapy, surgery, immunotherapy. Introduction
Urinary Injury • Urethral Injury • Bladder Injury • Urteric • Kidney Injury • Iatrogenic Vs traumatic
Urethral Trauma • Almost exclusively in male • Significant morbidity • Stricture • Incontinence • Impotence • If unrecognized: • Converting partial to complete tear • Foley catheter implication
Anatomy Prostatic Bladder Symphysis
Posterior Urethra • Violent external force • Pelvic fracture in 90% • Gross hematuria in 98% • Inability to void • Blood at urethral meatus • Pelvic / suprapubic tenderness • Penile / scrotal / perineal hematoma • Boggy / high-riding prostate/ ill-defined mass on rectal examination
Diagnosis:Retrograde Urethrogram • Pretest KUB film • Supine position • Injection of 25ml of water-soluble contrast • Post-voiding x-ray.
Retrograde Urethrogram:Interpretation • Contrast extravasation + Contrast in bladder • Contrast extravasation only PARTIAL Tear COMPLETE Tear
Partial Tear • careful passage of 12-14 Fr. Foley. • If any resistance:Suprapubic catheters Surgical approach / Endoscopy Delayed repair usually
Complete Tear Suprapubic catheters. Surgical approach / Endoscopy Delayed repair usually • If Foley already there and suspected • LEAVE FOLEY IN PLACE
Anterior Urethra • More common than posterior • Direct trauma • Usually NO pelvic fracture • Blood at meatus • Unable to micturate • Penile/Scrotal/Perineal • Contusion • Hematoma • Fluid collection • NO Foley if injury suspected • Retrograde Urethrogram • Surgical Treatment
Bladder Trauma • Adult: Extraperitoneal organ • Bladder dome = weakest point • Blunt: 60-85% • Important to recognize • Pelvic/abdominal wall abscess/necrosis • Peritonitis • Sepsis / Death
Types of rupture • Extraperitoneal • Most common • Pelvic fracture in 89-100% • Intraperitoneal • Extravasation of urine in abdomen • Sudden force to full bladder • Associated injuries • Mortality (20%) Investigation • US • Cystography: Gold standard • CT Cystography : New trend • ABCD for polytrauma • Exeploration and repair
Kidney Injury • Kidney is : Retroperitoneal organ Cushoned by perinephric fat and Gerota’s fascia Along T10 - L4 Ribs 10-12 Fixed only through pedicle. • Blunt trauma: 80-90% • MUST be suspected if • Trauma to back / flank / lower thorax / upper abdomen • Flank pain / low rib fracture • Hematuria / Ecchymosis over the flanks • Lumbar transverse process fracture
Investigation • IVP • Used to be intial exam of choice. • Very poor sensitivity for penetrating injury • Limitation in staging renal injuries • Not 1st choice anymore. Only if pt unstable. • Contrast CT • Study of choice if stable • More sensitive and specific for staging • Detects other abdominal injuries
Management… • Absolute indication for Surgery: • Uncontrollable renal hemorrage • Multiply lacerated, shattered kidney • Main renal vessels avulsed • Penetrating injuries usually • Grade I-II • conservative • Grade III-IV • Conservative if stable hemodynamically vs. surgery • Grade V • Surgery
Causes of Obstructive Uropathy Anatomical Obstruction within the lumen in the wall out side Pathological congenital tumor trauma inflammation vascular others
• Urinary Tract Obstruction: • Recognition of obstruction is important since it increase the chance of infection and stone formation. In addition unresolved obstruction almost always lead to permanent renal atrophy fortunately many causes of obstruction are surgically correctable or medically treatable. • It can be sudden or insidious, partial or complete, unilateral or bilateral. It may occur at any level of the urinary treat from the urethra to the renal pelvis. • It can be caused by lesion that are intrinsic to urinary tract or extrinsic lesion that compress the ureter.
Urinary Tract Infection Definition Women: Presence of at least 100,000 colony- forming units (cfu)/mLin a pure culture of voided clean-catch urine Men: Presence of just 1,000 cfu/mLin a pure culture of voided clean-catch urine indicates urinary tract infection
Risk Factors for UTI • Female, • Advanced Age, • Fecal incontinence/impaction, • Incomplete bladder emptying or neurogenicbladder, • Vaginal atrophy/estrogen deficiency, • Pelvic prolapse / cystocele, • Insufficient fluid intake/dehydration, • Indwelling Foley catheter or urinary catheterization or instrumentation procedures, • Diabetes or immunosuppression, • Benign prostatic hypertrophy • Bladder or prostate cancer, • Urinary tract obstruction • Spinal cord injury
Causative Pathogens • Escherichia coli — gram (-) etiologic agent in ~ 80% of all UTI’s • Source of microbial invasion is retrograde colonization Polymicromialbacteriuria • Contamination most frequent cause of multiple microorganisms • Sours :fistulas, urinary retention, infected stones, or catheters
Symptoms versus Asymptomatic Bacteriuria Asymptomatic Bacteriuria (ASB) • Defined as the presence of bacteria in urine of patients who do not have dysuria, urinary frequency, urgency, fever, flank pain, or other symptoms related to irritation of the urethra, bladder, or kidney • Strictly defined—exists when 2 urine cultures done with clean-catch specimens are positive in a patient who has no urinary tract symptoms signs and Symptoms • Dysuria, urinary frequency, urgency • Clarity of urine • cloudy, milky or turbid → bacteriuria • Cloudiness, however, can occur in normal urine—mucus, epithelial cells • Cloudy character, alone or with (+) dipstick analysis → further lab analysis • Bloody • Hematuria not always indicative of infection; possibly irritation or medication related • Malodorous • Pain • Despite limitations of assessment in the elderly, suprapubic, flank or CVA pain can indicate UTI • Incontinence • May be caused by UTI or the altered mental status that that occurs with the elderly Elevated temperature
Diagnostic Criteria Pyuria • Associated with presence of both symptomatic and asymptomatic UTI’s in elderly • Level of pyuria is ↑ when infected with a gram negative organism
Laboratory Analysis Dipstick Testing Used in primary care & LTC settings. But for institutionalized adults, urinalysis is preferable. • Chemically impregnated reagent strips (UA Chemstrip Screen) provide preliminary/quick determinations of: pH bilirubin protein blood glucose *nitrite ketones *leukocyte esterase urobilinogen specific gravity Routine Urinalysis—Key Indicators of Infection • Urine collection 1st morning specimen is best • Appearance Cloudy, may not indicate WBC’s • Odor Normal → faint odor when freshly voided Foul-smelling—often presence of bacteria which splits urea to form ammonia • pH control of pH → manages bacteriuria, renal calculi & drug Rx • Blood Always an indicator of kidney/UT damage • WBC’s
Laboratory Analysis • Urine Culture and Sensitivity Traditional gold standard for significant bacteriuria >100,000 cfu/mL of urine. • Complete Blood Count with Differential • Indicated to R/O bacterial infection supports treatment plan Careful evaluation of WBC & differential (left shift) • Electrolytes • R/O dehydration & if IV fluids replacement needed • BUN, Creatinine • Determine ↓ renal function for nephrotoxic medications • Blood Culture • Identify bacteremic organism in suspected urosepsis
Treatment Plan • Early detection to prevent systemic infection, bacteremia • Initiation of antibiotic treatment is recommended for a clinically-diagnosed UTI. • AB for at least10 days, as short-term therapy, may not be as effective. • Ten-14 days, if indicated, for complicated UTI. • Adjust medication when urine C&S is final • Selection of antibiotic must be individualized and consider: • Side effect profile • Cost • Bacterial resistance • Likelihood of compliance (convenience, fewer pills/day ↑’s compliance) • Effect of impaired renal function on dosing • Possible adverse drug reactions ↑ in elderly (multiple drugs, co-morbidities.
Prevention Indwelling-Catheterization Foley catheterization should be avoided if at all possible • Most effective means of UTI prevention is limitation of chronic indwelling catheters.
Prostate • Anatomy – 5 lobes. • Median/Posterior – (BPH/Cancer) • Hormone response – Estrogen like • Enlargement – Inflammation / growth • Neoplastic / Non neoplastic growth. BPH / Cancer.
BPH Bignin Prostatic Hyperplasia • Common non-neoplasticEnlargement. • Involves peri urethral zone. • BPH is common as men age. • 75% among men aged 70-80years • Over 90% in people aged over 90y • Rare before the age of 40y.