Pulmonary Tuberculosis
Pulmonary Tuberculosis. Evolution and Clinical picture. Global burden of TB . In 1993 WHO declared TB a global emergency . It is estimated that 9 million new cases of TB occurred /year and 3 million TB deaths/year . Tuberculosis poses a major problem for developing countries .


Pulmonary Tuberculosis
E N D
Presentation Transcript
Pulmonary Tuberculosis Evolution and Clinical picture
Global burden of TB • In 1993 WHO declared TB a global emergency . • It is estimated that 9 million new cases of TB occurred /year and 3 million TB deaths/year. • Tuberculosis poses a major problem for developing countries . • 75% of TB cases in developing countries are in the economically productive age group ( 15-50 ys)
Why does the global burden of TB increase? • Improper management • Impact of HIV pandemic • Poverty, drug addiction and an increasing number of homeless people .
Etiology: • Mycobacterium tuberculosis • Three types can infect man: • The human type: the commonest type. • The bovine type. • The atypical or opportunistic mycobacteria.
Mode of infection • The disease is transmitted through inhalation of infected sputum droplets or ingestion of infected milk .
Primary Tuberculosis • Occurs in the body when it is infected for the first time . • Usually in children • It can occur in adults who are exposed for the first time . • Occasionally typical primary TB occur in elderly people who lost their tuberculin sensitivity
Pathology: • The characteristic lesion is the tubercle. • It consists of a collection of epithelioid cells surrounded by lymphocytes, fibroblasts and giant cells with bacilli in the center • The primary tuberculous infection usually occurs in the lung but occasionally in the tonsils or in the alimentary tract.
Characteristics of primary tuberculous lung lesion (primary complex): • Usually in the lower part of the upper lobe or in the upper part of the lower lobe commonly on right side (Ghon’s focus) • Coexisting endobronchitis and lymphangitis. • Caseous lymph nodes.
Inchildren the nodal component is more obvious than lung component. • In adulthood prim TB the lung component is more evident & located more in upper lobes, (that is why it is not easy to distinguish between prim and postprim in adults unless recent tuberculin conversion has been documented).
Allergic reaction: • Appears against the protein part of the bacillus. • reflected pathologically as caseous necrosis by the 2nd wk.
Immunologically manifested by : • Hypersensitivity(tuberculin reaction & other hyperergic manifestations) • +ve tuberculin is the earliest indicator of infection by TB (6th wk) • -ve reaction does not exclude infection by TB • Immunity or resistance • mediated by T lymphocytes which on contact with antigen produces lymphokines which activates macrophages so that it phagocytose & destroy bacilli at a markedly enhanced rate compared to nonstimulated cells
Both hypersensitivity and immunity develop simultaneously • Cell mediated type IV reaction is responsible for both phenomena.
Protective immunity (PI) Vs delayed hypersensitivity (DH) in pathogenesis of TB • The observation that advanced TB is associated with –ve tuberculin gave the questionable impression that +ve tuberculin means good immunity. • However, the current concept is that PI & DH are separate immunologic events. • In PI monocytes are recruited, activated to destroy intracellular bacilli and differentiate into epithelioid cells forming the granuloma. This is mediated by protective CD4 T cells (TH1) • In DH non activated macrophages are killed, caseation occurs followed by liquefaction , cavitation , extracellular bacillary multiplication morbidity & infectivity. This is mediated through cytolytic CD4 cells (TH2)
Methods of spread of TB infection • Local spread: bacilli being taken by epithelioid cells to surrounding tissue to form new tubercles. • Lymphatic spread to regional lymph nodes specially in prim infection • Blood born spread: •Early in prim infection bacillemia occurs through lymph-hematogenous spread with seeding of bacilli to all parts of the lungs and also other body organs. •These dormant foci are reactivated later on with marked potential variability according to local and general resistance.
I.Fate of primary focus (lung component) • (1)Good fate (regressive primary) •Regression occurs when: Low virulence of bacilli High host resistance •Resolves & disappear completely by absorption •Healing by fibrosis, calcification & even ossification •Some bacilli may be imprisoned alive and become active again when resistance decreases
(2)Bad fate (progressive primary – one type of postprim tuberculosis) • Occurs when high virulence or dose of bacilli low host resistance •Local extension pneumonia, cavitation pleural effusion •Hematogenous dissemination bronchial vein Rt side of Ht lungs pulmonary vein Lt side of Ht allover the body pulmonary artery one lung dissemination
II.Fate of primary focus (glandular component) (1)Good fate (regressive primary) as lung component (2)Bad fate (progressive) (1)Bronchial complications compression Þ brassy cough partial obstruction Þ emphysema complete obstruction Þ collapse erosion Þ aspiration (2)Rupture in blood vessel Þ hematogenous spread
Clinical features: • Symptomless, • brief febrile illness at the time of tuberculin conversion that is indistinguishable from the many febrile illnesses of childhood. Most children are symptom-free and are discovered only when they are investigated as contacts of an adult case, • may occur in elderly people who have lost their tuberculin sensitivity. • In most cases there are no detectable physical signs. • the child may be unwell with loss of appetite, fretfulness and failure to gain weight.
• Cough is not usual but may occur, and may mimic the paroxysms of whooping cough when lymph nodes or tuberculous granulation tissue impinge on the bronchial wall; • wheeze. • Sputum production is rare in children. • Auscultation of the chest occasionally crepitations may be heard over an extensive primary focus. • More obvious physical signs may be present if there is segmental or lobar exudation or collapse.
Hyperergic manifestations of Tuberculosis - Post. tuberculinreaction. - Epituberculosis • This term is not used now • It describes dense homogenous shadow in lung of children with tuberculosis. •This radiological appearance is due to - hypersensitivity reaction to tubercle protein - tuberculous pneumonitis (rarely caseating) - collapse by pressing lymph node pouring of caseous material caseous bronchitis and stenosis - Erythemanodosa. -Phlyctenular conjunctivitis. - Allergic pleural effusion.
Other sequela of prim. TB • Broncholith • Calcified primary or lymph node extruded to bronchus hemoptysis • Bronchiectasis mostly in upper lobe. • Obstructive emphysema • external pressure or endobronchitis valve like mechanism
Radiological features • • Radiological changes are found at the time of tuberculin conversion in 7-30% of young adults. • • Lymphadenopathy. The hilar lymph node was most commonly involved but the paratracheal node was also frequently enlarged. • • Bilateral hilar adenopathy may be seen. In adults the lung component of the primary complex is usually more obvious and the nodal component may not be seen. • Radiological abnormality persists in a majority 6 months after diagnosis but complete resolution is usual after 2 years. • Usually after a year or more but rarely, the lung or nodal component of the primary complex or both may calcify. Calcification may occur in the absence of any chest radiographic changes in the acute stage.
POST PRIMARYTUBERCULOSIS • Infection occurring after sometime from the primary infection. • Tissue reaction is different from that in prim reaction because the ground has been changed by acquired immunity & hypersensitivity. • Unlike prime disease, postprim bronchogenic TB is characterised by increased local destruction caseation and cavity formation while lymph nodes enlarge rarely and lately (if suppressed immunity). • This is because enhanced phagocytic activity prevents spread to lymph nodes aiming at localising infection and destroying bacilli.
HEMATOGENOUS TB A disease caused by dissemination of tubercle bacilli via blood to involve more than one organ not related to each other except by blood stream.
Source of bacillemia • - Progressive primary. • - During advanced bronchogenic TB • - Surgery on tuberculous origin (curettae of endometritis, massage of arthritis) • so surgery should be under anti TB cover • Tuberculous endangitis : Seeding of bacilli into vessel walls may cause a caseous vasculitis of the intima , with subsequent discharge of bacilli into the blood stream leading to miliary spread. Usually solitary, caseating and liquefying but can later heal by endothelial covering. Can occur in large veins & thoracic duct but less commonly in arterial system.
Forms of dissemination acute : Large no of bacilli + poor resistance chronic: small no of bacilli + good resistance takes months or years to develop
Acute Miliary TB • Characterised by millet seed sized foci uniformly distributed throughout the lung or other involved organs. • A typical tubercle structure is not commonly seen in acute form unlike the chronic. • The more acute the less pronounced the caseous reaction.
Clinical features Acute or classical miliary tuberculosis • The disease is most common in infants and young children. • In children, the onset may be associated with an acute or sub acute febrile illness • In adults, the onset is insidious with gradual development of vague ill-health, malaise, anorexia, weight loss and fever. • Cough, breathlessness, haemoptysis and night sweats are less common. • Headache as a feature suggests associated tuberculous meningitis, which is found in an appreciable proportion of cases.
No physical signs. • The chest is frequently normal on auscultation, although crepitations may develop in the later stages. • Hepatomegaly, nuchal rigidity, lymphadenopathy and splenomegaly may be found in a proportion of cases. • Choroidal tubercles are found in over 90% of children with miliary tuberculosis but less commonly in adults. • Miliary lesions of the skin are very occasionally seen and may take the form of macules, papules, vesicles or purpuric lesions.
Cryptic miliary or disseminated tuberculosis • A variant pathological type known as ‘non-reactive’ • The lesions are mainly necrotic, with no obvious tuberculous histology, and are teeming with tubercle bacilli. The spleen and liver may be enlarged and studded with irregular necrotic foci, usually less than 1 cm in diameter or only visible microscopically. Any organ may be affected. • Increasingly being seen in the elderly, where it may be difficult to diagnose since the chest film may be normal, choroidal tubercles are absent and the tuberculin test may be negative.
The most common presentation is with the insidious onset of weight loss, malaise and a fever of unknown origin. Anemia is usual and the ESR is often elevated. A variety of blood dyscrasias, including leucopenia, pancytopenia, aplastic anaemia, leukemoid reactions leucoerythroblastic anaemia and polycythemia, have been seen. • The liver function tests are commonly disturbed, with elevation of transaminases and alkaline phosphatase. Hyponatremia and hypokalemia are also commonly seen.
Radiology • chest radiograph may be quite normal in the presence of miliary tuberculosis, since the lesions are too small to be seen. • abnormal shadows are usually fairly evenly distributed and may vary from faint shadows 1-2 mm in diameter to large dense shadows up to 5 or 10 mm. • Usually the shadows are all a similar size but, as the disease processes, larger coalescent shadows may develop. • Evidence of a primary tuberculous complex, complicating segmental lesion or a postprimary lesion may be seen. • Bilateral pleural effusion may occur.
Chronic haematogenous spread Pathologically characterized by : • tendency to fibrosis & calcification. • caseation plays a minor role • restriction of spread to certain areas (bronchi are rarely involved) • presence of extra pulmonary lesions. Radiologically : • symmetrical distribution • uniformity of size fo the lesions • ± calcification or bilateral pleural effusion.** Clinically : • General toxemia • Lack of local signs & symptoms (cough, expect, hemoptysis are not usual)
Pulmonary manifestations of chronic haematogenous TB (1)Chronic miliary dissemination sharply defined foci with typical tubercle structure connected with fibrotic strands (2)Corticopleural dissemination groups of foci are seen at the margin of one lobe beneath & implicating the pleura (3)Disseminated emphysematous type characterised by fibrosis alveolar dilatation emphysema & bullous formation (bullae alternating with fibrosing military nodules) (4)Punched out cavities •thin walled stamped out cavities •no sputum as necrotic material is absorbed by blood rather than expectorated •either heal or persist as thin walled spaces over years. •differ from cavities of bronchogenic TB that show thick fibrosed walled & caseation. (5)Simmon’s foci •large apical foci with caseating or calcified centers surrounded by fibrosed lung and covered by fibrosed pleura (fibrosa densa) •usually multiple
Extra Pulmonary manifestations of chronic haematogenous TB • Intrathoracic 1-bilateral hilar (& other mediastinal glands??) 2-pericardial 3-pleural • Extrathoracic 1-urogenital 2-bone & joint 3-CNS tuberculomata 4-lymph nodes 5-serous membranes & meninges
Postprimary pulmonary tuberculosis Bronchogenous TB • Postprimary pulmonary tuberculosis is by far the most important type of tuberculosis, partly because it is the most frequent and partly because smear-positive sputum is the main source of infection responsible for the persistence of disease in the community. • It is usually present in upper lobes and is often bilateral as it starts in one lung and spread via bronchi to other lung .
Pathogenesis • Postprimary pulmonary tuberculosis may arise in one of three ways: • direct progression of a primary lesion; • (ii) reactivation of a quiescent primary or postprimary lesion; • (iii) exogenous reinfection.
Factors helping reactivation of TB lesion • Bad housing, overcrowding ,Cigarette smoking , Alcoholism & addiction • Fatigue, malnutrition & debility • Silicosis through toxic effect on macrophage • Health service professions • Diabetes millets • Steroids & immunosuppressants • Lymphomas, leukaemia, AIDS • Gastrectomy, peptic ulcer, vagotomy • Hepatobiliary disease • Pulmonary stenosis oligemia TB • (mitral stenosis decrease incidence due to plethora) • Lung cancer developing in TB focus
Pathological picture depends on interrelationship between • virulence of bacilli • hypersensivity of the host • local O2, CO2 & blood flow
2 forms may occur 1- apical reaction with fibrosis with or without calcification living bacilli will be left in this focus & may cause bacillemia later on. 2- chronic fibrocaseous TB The Rt lung is more affected (usually subapically i.e. post. Seg. Of UL & apex of LL) Lower lobe TB is common in: Diabetes Negroes pregnancy • Cavitation occurs • The pleura may be involved either as • TB pleurisy , Visceroparietal adhesion • Hilar nodes not enlarged
Clinical features • The majority of patients are middle-aged or elderly. • no symptoms • gradual onset of symptoms over weeks and months • general symptoms, such as tiredness, malaise, loss of appetite, • weakness or loss of weight. • febrile symptoms may be reported and night sweats • Cough : • persisting for more than 3 weeks, should have a chest radiograph. • Sputum may be mucoid, purulent or blood-stained • Haemoptysis is a classic symptom , massive haemoptysis is usually • due to erosion of a bronchial artery, which bleeds at systemic pressure.
Physical signs • no physical signs in spite of extensive radiological changes. • post-tussive crepitations in the upper zones or apices. • There may be signs of consolidation. • In chronic disease, deviation of the trachea may occur due to fibrosis. • The classical physical signs of a cavity are seldom found even when large cavities are evident on the chest film. • Localized wheezes may occasionally be heard if the patient has severe endobronchial tuberculosis.
In general, examination of the chest contributes relatively little to the diagnosis or assessment of postprimary tuberculosis. Sputum examination and chest radiography are much more important. However, it is essential to conduct a general examination of the patient as there may be additional tuberculous lesions outside the chest.
Radiology • It is possible for a patient to have localized postprimary endobronchial tuberculosis with a positive sputum and a normal chest film. • Pulmonary tuberculosis can mimic almost all other pulmonary diseases.
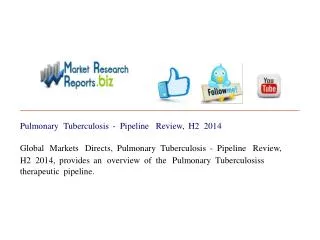
Appearance suggestive of tuberculosis : The following characteristics of a chest radiograph favour the diagnosis of tuberculosis : 1.opacities mainly in the upper zone(s); 2.patchy or nodular opacities; 3.presence of a cavity or cavities; 4.presence of calcification; 5.bilateral opacities especially if in upper zones; 6.opacities that persist after several weeks (and thus are less likely due to acute pneumonia).
No chest x-ray pattern is absolutely typical of pulmonary TB .