Download
1 / 74
740 likes | 1.58k Vues
Reminder Dialogs and National Reporting . Session # 227. Faculty. Charles Zeilman, III, PhD, ARNP, BSN, Chief Clinical Informatics Service Russell Jacobitz, BSN, RN Operations Manager Clinical Informatics Service Karl Sault, BSN, RN Clinical Applications Coordinator Debbie Trost

E N D
Reminder Dialogs and National Reporting Session # 227
Faculty • Charles Zeilman, III, PhD, ARNP, BSN, • Chief Clinical Informatics Service • Russell Jacobitz, BSN, RN • Operations Manager Clinical Informatics Service • Karl Sault, BSN, RN • Clinical Applications Coordinator • Debbie Trost • Clinical Reminder Project Analyst, OI&T SLC
Overview • Demographics • Performance Measures • Oryx • Hedis • Directives/Informational letters • Clinical Reminder System • Implementation • Reporting/Feedback • What’s Ahead for Reminders Package?
NFSG Demographics Jackson County CBOC in Marianna, Florida Fiscal Year ’08 Camden County CBOC near St. Mary’s, Georgia Fiscal Year ’08 Putnam County CBOC near Palatka, Florida Fiscal Year ’09 South Marion County 90,000 SF Specialty Construction FY '08 Activation FY ’10 • 10 facilities (Clinical care provided for 2 additional Orlando facilities: Daytona Beach and Leesburg) • 2 Medical Centers with OPCS, 2 OPCS, & 6 CBOC’s • 3 Future Facilities • 124,720 uniques (FY2007) • 1.3 million visits (FY2007)
Chief of Staff ACOS, Quality Management Clinical Informatics Program Support Assistant Chief, Clinical Informatics Lake City VAMC Staff CPRS Support/Education 0.5 CAC 0.5 CPRS Operations Manager Consult/Procedure Facilitator Vacancy Clinical Application Coordinators Clinical Informatics Clinical CPRS Educator (GV) CAC CAC CAC CAC CAC Organizational Chart Clinical Informatics Service
Performance Measures • Oryx • Measures developed by Joint Commission to meet the data reporting requirement associated with accreditation. Based on workload and mission, an accredited facility may use (3) core measures (AMI, PN, HF, SIP) or (9) non-core measures (developed by the organization) or a combination of both. Joint Commission will want to see data and QI as it relates to the ORYX measures. • Hedis • Health Plan Employer Data and Information Sets - a set of standardized performance measures designed to ensure that purchasers and consumers have the information they need to reliably compare the performance of managed health care plans
Directives and Informational Letters • Directives • Establish mandatory VHA policies • Example- VHA DIRECTIVE 2007-004 COLORECTAL CANCER SCREENING • Informational Letters • Release nondirective information of one-time interest or short duration; i.e., applications for training opportunities, describing new programs, announcing meetings, reminders etc. • Example- ABDOMINAL AORTIC ANEURYSM (AAA) SCREENING IL 10-2007-011
Process for Colorectal Cancer Screening • Discussion of Directive: • VHA DIRECTIVE 2007-004 COLORECTAL CANCER SCREENING • Screening Test Options • Positive Screening Test • NFSG VHS Process
VHA DIRECTIVE 2007-004 • COLORECTAL CANCER SCREENING • Screening Tests: a. Home fecal occult blood test (FOBT) alone every year (three consecutive stool samples). b. Flexible sigmoidoscopy alone every 5 years. c. Home FOBT every year combined with flexible sigmoidoscopy every 5 years. d. Double Contrast Barium Enema (DCBE) every 5 years. e. Colonoscopy alone every 10 years.
VHA DIRECTIVE 2007-004 • Positive Screening Test • “For any positive screening test, the provider responsible for initiating follow-up must develop a follow-up plan or must document that no follow-up is indicated, within 14 calendar days of the screening test (day of laboratory receipt of FOBT, day of test for sigmoidoscopy, or DCBE). If a diagnostic colonoscopy is indicated, the colonoscopy must be performed within 60 calendar days of the positive screening test.”
VHA DIRECTIVE 2007-004 • Positive Screening Test • “FOBT results (positive) must be conveyed to the patient in writing or orally within 14 calendar days from day of laboratory receipt of FOBT” • “Written reports of verbally-transmitted positive test results must be sent to the patient within 14 calendar days of the test date, unless the patient has already been scheduled for follow-up of the positive test.”
NFSG Process Colorectal Cancer Screening • Collaborated with Key Stakeholders • Associate Chief of Staff for Quality Improvement (Performance Measures) • Chief, Clinical Informatics Service • Gastroenterology Section • Ambulatory Care Service
NFSG Process Colorectal Cancer Screening • Issues • Consistent documentation FOBT positive results and plan of care. • Volume of FOBT positive lab results. • Monthly average of 250 Positive FOBT Lab results. • Identification of FOBT positive consults for colonoscopy. • Volume of colonoscopy requests. • Monthly average of 940 colonoscopy consults. • Correlated to 250 (27%) FOBT Positive colonoscopy consult requests.
NFSG Process Colorectal Cancer Screening • Issues • Tracking and reporting of documentation for FOBT positive lab results and plan of care. • Patient notification of positive screening test (FOBT) result. • Tracking and reporting of consult completion time.
Process for AAA Screening • Discussion of Informational Letter: ABDOMINAL AORTIC ANEURYSM SCREENING IL 10-2007-011 • Recommendations from the VA National Center for Health Promotion and Disease Prevention (NCP): • Men between the ages of 65 and 75 who have ever smoked need to be offered one-time screening for AAA, preferably with ultrasonography. • Repeat Screening Recommendations: • AAA Size less than 3.0 cm (normal) do not need repeat screening. • AAA Size 3.0 to 3.9 cm need to be followed every 2-3 years. • AAA Size 4.0 to 5.4 cm need to be followed every 6 months. • AAA Size greater than 5.5 cm, referral for surgical intervention needs to be considered.
NFSG Process AAA Screening • Collaborated with Key Stakeholders • Associate Chief of Staff for Quality Improvement (Performance Measures) • Chief, Clinical Informatics Service • Surgical Service Chief and Vascular Section Chief • Ambulatory Care Service • Radiology Service • OIT-Local CPRS Programmer
NFSG Process AAA Screening • Issues • Deployment of AAA Reminder for Screening. • Pilot at Gainesville Facility to estimate demand on Vascular Service Consults and Radiology US & CT Scans. • PCP Follow up Screening for Positive AAA. • Tracking and reporting of positive screening to meet clinical standards. • Concern for demand on Vascular Consult Service.
Russell Jacobitz BSN, RN • Reminder Dialogs as a Solution • The Clinical Reminder System • Overview of reminders • Advantages of using dialogs • Application in regards to mentioned directives/initiatives • Templates • Form Letters
The Clinical Reminder System • Clinical Reminders Overview: • “The Clinical Reminder system helps caregivers deliver higher quality care to patients for both preventive health care and management of chronic conditions, and helps ensure that timely clinical interventions are initiated.” • Primary goal to improve care for Veterans • Assists in clinical decision-making, documentation and follow-up • Place relevant orders within the reminder Clinical Reminders Version 2.0 Patch PXRM*2*4 CLINICIAN GUIDE October 2006
The Clinical Reminder System • Benefits for Clinical and Administrative Purposes: • Provides data for clinical decision-making • Reduces duplicate documentation • Targets special patients populations • Assists with compliance with VHA performance measures • Assists with Health Promotion and Disease Prevention guidelines.
The Clinical Reminder System • Reminder Dialogs • “Reminder Dialogs comprise a predefined set of text and findings that together provide information to the CPRS GUI, which collects and updates appropriate findings while building a progress note.” Clinical Reminders Version 2.0 Patch PXRM*2*4 CLINICIAN GUIDE October 2006
The Clinical Reminder System • Functionality • Can be linked to the following • Clinical Reminder • Shared Template • Progress Note Title • Advantages • Ability to pass information into record • Ability to track, collect and report data • Ability to enter orders from the notes tab
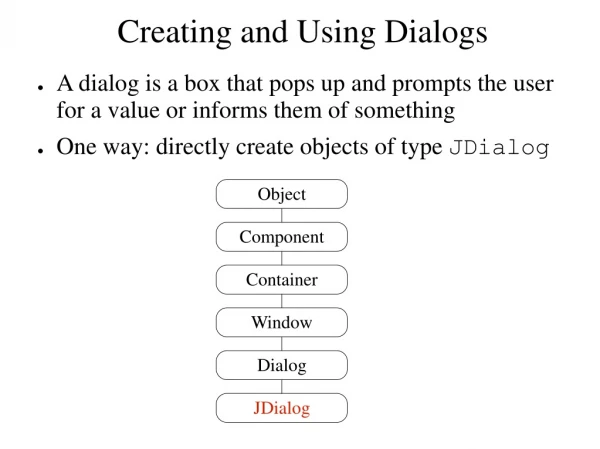
Dialog Components Components of the dialog include the point and click area for documentation, the progress note text, and the information being passed to the record.
Form Letters • Patch TIU*1*222 SEQ #217 • TIU Work Copy Modification & Form Letter Functionality • Brief discussion applying to today's process.
Karl Sault BSN, RN, CAC • NFSG VHS AAA Screening and F/U Process • Utilizing a combination of tools: • Computed Finding • Radiology Reports • Reminders
Computed Findings • “Computed findings provide the ability to create custom findings for situations when none of the standard findings will work.” • Computed Finding (CF): • Radiology created standardized report. • Local CPRS Programmer created CF based on the standardized report. • CF utilized in reminders to resolve or initiate follow-up care. Clinical Reminders Manager Manual December 2007