Download
1 / 30
930 likes | 3.48k Vues
This presentation focuses on the importance of human factors in anaesthesia practice and introduces the principles of the Helsinki declaration for patient safety.

E N D
Safety in anaesthesiaThe Anaesthetist’s Task Tarek Samir Shabana Lecturer of Anaesthesia Ain Shams University
Objectives : • Understanding the importance of human factors in anaesthesia practice • Identifying limitations of human factor • Introducing the principles of the Helsinki declaration for patient safety • Understanding the value of incident reporting in creating apatient safe culture
“ It is not the drug that is dangerous, but the man who administers it is” Sir Robert Macintosh
Human factor I. Technical skills such as intubation or central venous access, are taught and assessed II. Non-technical skills Including situational awareness, decision-making, leader ship, teamwork and communication
Human factor limitations • Fatigue, stress • Surrounding atmosphere • Increasingly complex systems • Lack of communication
Pre-Use Preparation and Checkout of Equipment • Infusions • Syringe labelling • Life support equipment • Anaesthesia machine and ventilator
The FDA Recommendations for Anesthesia Apparatus Checkout • Emergency ventilation equipment • High pressure system • cylinder half-filled ( 1000 psi) • central pipeline supply hoses connected, gauge reading 50 psi 3. Low pressure system Check initial status : turn vaporizer off, check level and tighten cap
The FDA Recommendations for Anesthesia Apparatus Checkout 4. Perform leak check (universal negative pressure leak test)
The FDA Recommendations for Anesthesia Apparatus Checkout 5. Turn master switch on 6. Flowmeters (full range, hypoxic guard) 7. Scavenging system 8. Calibrate O2 sensors Expose to room air and allow to equilibrate (2 min). Then expose to oxygen source and ensure it reads near 100% 9. Check breathing system 10. Perform leak check for breathing system Minimal gas flow close APL occlude Y piece O2 flush till 30 cmH2O ensure pressure fixed for 10 sec
The FDA Recommendations for Anesthesia Apparatus Checkout 11. Check ventilation systems and unidirectional valves 12.Check, calibrate, set alarm limits of all monitors 13.Final status of machine: • Vaporizers off • Bag/Vent switch to "bag" mode • APL open • Zero flows on flowmeters • Suction adequate • Breathing system ready
Syringe labelling Medication errors are the second most common category of incident reported to the NPSA Cousins D, Gerrett D, Warner B. A review of medication incidents reported to the National Reporting and Learning System in Englandover six years (2005–2010). .
Patient Identification Use at least two identifiers (e.g. name and date of birth) , neither of them should be the patient’s room number
ASA standards for basic anaesthetic monitoring • Qualified provider throughout anaesthesia • Oxygenation : O2 analyser / oximeter • Ventilation : Capnography / ventilator alarms • Circulation : ECG /BP • Temperature + Observe ( colour/ chest movement/ blood loss)
Anaesthetic record . The anesthetist must keep a good record of the course of anesthetic; otherwise it will be difficult to defend a case should things go wrong
Postoperative AAGBI safety guidelines 2013 • PACU after general, spinal or epidural • Monitored / observed (1:1) • Trained nurse • Discharged only by anaesthesiologist • Written criteria for discharge
The Helsinki declaration for patient safety in anaesthesiology Prepared jointly by The European Board of Anaesthesiology (EBA) and the European Society of Anaesthesiology (ESA). It was launched in June 2010 at the Euroanaesthesia meeting in Helsinki.
1. All institutions providing perioperative anaesthesia care to patients should comply with the minimum standards of monitoring recommended by the EBA both in operating theatres and in recovery areas.
Pulse oximeter • NIBP • ECG • Temperature • Airway gases (CO2, O2, vapor) • Airway pressure • Nerve stimulator ( if muscle relaxants are used)
2.All such institutions should have protocols and the necessary facilities for managing the following : A.Preoperativeassessment and preparation B.Conductof anaesthesia • Checking Equipment and drugs • Syringe labelling • Difficult/failed intubation • Malignant hyperpyrexia • Anaphylaxis • Local anaesthetic toxicity • Massive haemorrhage • Infection control C.Postoperative care including pain relief
3. All institutions providing sedation to patients must comply with anaesthesiologyrecognised sedation standards for safe practice.
4. All institutions should support the WHO Safe Surgery Saves Lives initiative and Checklist
. 5.All departments of anaesthesiology in Europe must be able to produce an annual report of measures taken and results obtained in improving patient safety locally. 6. All institutions providing anaesthesiological care to patients must collect the required data to be able to produce an annual report on patient morbidity and mortality. 7. All institutions providing anaesthesiological care to patients must contribute to the recognised national or other major audits of safe practice and critical incident reporting systems. Resources must be provided to achieve this
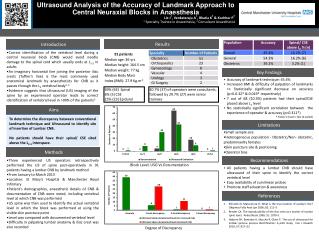
The closed claim project(University of washington, seattle)In depth investigation of closed insurance claims
TAKE HOME MESSAGE 1.Continuous Training, education and assesment 2. Protocols (preoperative, intraoperative, postoperative) 3.Comply with standards of anaesthesia care 4. Incident reporting