Download
1 / 39
390 likes | 646 Vues
Conservative Interventions for Treatment of Overweight and Obesity in Children. Deanna M. Hoelscher, PhD, RD, LD, CNS University of Texas Houston Health Science Center School of Public Health Human Nutrition Center/Center for Health Promotion & Prevention Research November 16, 2005.

E N D
Conservative Interventions for Treatment of Overweight and Obesity in Children Deanna M. Hoelscher, PhD, RD, LD, CNS University of Texas Houston Health Science Center School of Public Health Human Nutrition Center/Center for Health Promotion & Prevention Research November 16, 2005
Outline of Talk • Definitions & prevalence of child overweight • Why use conservative approaches? • Different methods • Diet • Protein Sparing Modified Fasts (PSMF) • Physical activity • Behavioral treatments • Use of pharmacologic agents • Conclusions/Recommendations
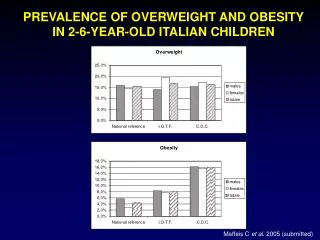
Overview of Child Overweight and Interventions • Overweight is defined as > 95th percentile based on CDC BMI chart • At risk of Overweight is defined as > 85thbut < 95th percentile based on BMI charts • The prevalence of overweight among children varies by gender and race/ethnicity • The prevalence of overweight is not a normal distribution, with skew to heavier weights • Primary aim of overweight interventions is energy balance (energy intake versus energy expenditure) • Very little data on preschool children • Practice is not evidence-based (not enough data)
How Do Children Differ From Adults with Regard to Weight Loss? • Reliance on parents as gatekeepers for food and physical activity • Consideration of growth and development from a biological standpoint • Cognitive/emotional development • Degree of overweight • School environment • Concern for eating disorders • Critical periods of adiposity increase (adiposity rebound, puberty) Source: Kirk et al., 2005
Rationale for Conservative Approaches to Child Overweight • Traditional view: • Overweight in children is benign or cosmetic • Children will “grow out” of overweight • Treatment paradigm: • Keep weight stable and let “grow into weight” • Weight loss, if any, should be modest so as to not affect growth and development • Use diet primarily, together with physical activity and behavioral counseling
Weight Gain for Children at the 75th Percentile from Age 6.5 to 18.5 OW/OW N/OW N/N Source: CDC weight charts, Butte & Ellis, 2003 OW = overweight, N = normal wt
Rationale for Conservative Approaches to Child Overweight • Current view: • Overweight in children is associated with both morbidity & mortality • Obesity in childhood leads to increased risk for severe obesity in adulthood • Child BMI tracks over time • With children at extreme weights (e.g., BMI >35), “growing into weight” is not an option • Treatment paradigms need to change Source: Dietz, 2004; Kirk et al., 2005; Baker et al., 2005; Kelder et al., 1994
How Growth and Weight Relate in Children over Time Source: CDC weight charts
Determination of Energy Intake in Children • To lose weight, need to determine how much change in energy intake • Difficult to determine energy intake in growing children • Estimates from Butte & Ellis, Science, 2003: • Deficit of about 300 kcal/day to prevent further weight gain in overweight children (range: 204-263 kcal/d) • Equates to 2, 12-oz sweetened beverages • Equates to walking about 60-120 minutes/day Source: Butte & Ellis, 2003
Conservative Interventions: Overview of Behavior Modification, Diet and Physical Activity Programs • Many diet and physical activity programs have behavior modification component • Most programs have all three components: behavior modification, diet and physical activity • Studies to date have mostly been conducted in clinic settings
Conservative Interventions: Diets in Children • Definition: Regulation of food intake either through change in macronutrient composition (e.g., fat, CHO content) or reduction in energy intake • Duration of treatment (in trials with adolescents): several weeks to 3 years • Maintenance of effects: Limited data • Compliance: Varies • Side effects: With Protein-Sparing Modified Fast (PSMF), protein losses, hypokalemia, hypoglycemia, inadequate calcium intake and orthostatic hypotension Source: Baker et al., 2005; Kirk et al., 2005
Conservative Interventions: Diets in Children • Weight loss achieved: 1-2 kg (2.2-4.4 pounds)/week, up to 1 kg/week with diet alone • Pros: Safe for more moderate diets • Cons: Usually involves a parent, costly, long-term, limited data on effectiveness, side effects for PSMF • Diets with altered macronutrient content (e.g., low glycemic load diets, low carbohydrate diets) have only been evaluated in small trials for limited periods of time. Source: Baker et al., 2005; Kirk et al., 2005
Example - Stop Light/Traffic Light Diet • Uses traffic light colors to characterize foods: • Green: low-calorie, high fiber foods, no restrictions • Yellow: essential foods, but because of higher nutrient density, eaten in moderation • Red: high in fat and/or simple sugars, limit to < 4 servings/d • Energy goals: 900-1300 kcal/d • Record all food and drinks • Adapted in various forms • Follows U.S. Dietary Guidelines where appropriate Source: Epstein & Squires, 1988
Promising Direction? Reduced Carbohydrate/Glycemic Load Diets • Ebbeling et al., 2003 • RCT, 6 month intervention and 6 month follow-up, n = 16 obese adolescents, aged 13-21 • Emphasized selection of foods with low to moderate GI, 30-35% energy from fat versus low-fat, 25 to 30% energy from fat • Difference of 2 kg/m2 • Spieth et al., 2000 • Retrospective cohort, n = 107 obese children, mean age about 10, mean length of time = 4 months • Low-GI diet versus standard reduced fat diet • Difference of 1.12 kg/m2 and 2.6 kg • Summary: relatively small studies, eliminate sugared beverages, sweets
Protein-Sparing Modified Fast (PSMF) • PSMF: around 1/5 g pro/kg IBW • For children, usually need a hospital stay, vitamins/minerals, K, calcium • Involves consistent monitoring of ketones • Gradual re-introduction of carbohydrates • Limited period of time (usually 3 months or less) • In one study with 8 adolescents (age 11-18), mean weight loss of 13.5 kg over 5 weeks • Published trials with children – few subjects, no RCTs Source: Brown et al., 1983; Merritt et al., 1981; Stallings et al., 1988
Conservative Interventions: Physical Activity/Sedentary Activity Interventions in Children • Definition: Programs designed to promote adolescent weight loss by increasing activity or decreasing sedentary behavior • Duration of treatment (in trials with adolescents): 3 months to 54 weeks (30-60 minutes/day for 3-7 days/week) • Maintenance of effects: No data • Compliance: Varies Source: Gutin et al., 2002; Owens et al., 1999; Epstein et al., 1995
Conservative Interventions: Physical Activity/Sedentary Activity Interventions in Children • Weight loss achieved: Difficult to quantify • Pros:Easier to maintain than diet over time, builds on usual child activities • Cons: Safety issues, time and money if parent is involved, sedentary activities are self-reinforcing Source: Gutin et al., 2002; Owens et al., 1999; Epstein et al., 1995
Examples of Physical Activity and/or Sedentary Activity Interventions • Owens et al., 1999 • 74 obese children (by TSF), 7-11 years old • 4 months training, 5 days/week, 40 min/day • Significant decrease in visceral adipose tissue (VAT) & total body fat mass (BMI not reported) • Gutin et al., 2002 • 80 obese (TSF), 13-16 years old • 8 month intervention, 5 days/week, 30 min/day • Significant decrease in VAT & % body fat • No differences between moderate and high intensity exercise
Conservative Interventions: Use of Behavior Modification in Children • Definition: Use of behavior modification strategies & counseling techniques (e.g., goal setting, stimulus control, etc.) in modifying dietary habits, physical activity patterns, addressing underlying psychological issues related to food and physical activity • Duration of treatment (in trials with adolescents): 1 session to 3 years (most are 4-6 months to 1 year) • Maintenance of effects: Follow up studies (1-10 years) show some maintenance effects • Compliance: Varies Source: Coates & Thoresen, 1978; Baker et al., 2005; Kirk et al., 2005
Conservative Interventions: Use of Behavior Modification in Children • Side effects: Few • Weight loss achieved: 4-15 pounds • Pros: Safe • Cons: Costly, long-term, personnel intensive, results are not consistent, involve considerable family involvement Source: Coates & Thoresen, 1978; Baker et al., 2005; Kirk et al., 2005
Examples of Successful Behavioral Interventions • Epstein work (Epstein et al.,1994, 1998, 1995) • 4 RCTs, n = 154 OW children, ages 6-12, 6 month treatment • Involvement of parents (family counseling) • Intensive family counseling not otherwise described • Long-term effects • 30% no longer overweight after 10 years • (5 years and 10 years) • Cons: specialized population (mostly white), omitted population with “psychological problems”
Promising Direction? Weight Loss Camps • Kirschenbaum DS, Craig R. • Wellspring camps (North Carolina, California, New York), ages 10-23 • www.wellspringcamps.com • Camps include diet, physical activity, behavioral therapy 4 x/week, family program, After-Care program online • Preliminary results- NAASO abstracts, 2005 • Mean weight loss = 1.78 kg/week • Weight loss continued during 6 month follow-up Source: Kirschenbaum et al., Obesity Res, 2005;13
Conservative Interventions: Use of Weight Loss Drugs in Children • Definition: Use of pharmacotherapy to lose excess body weight • Duration of treatment (in trials with adolescents): 3 months to 54 weeks • Maintenance of effects: No data • Compliance: For Orlistat, over 54 weeks, 65% remained in study • Side effects: Range from HTN to loose stools to risk of fat-soluble vitamin deficiency Source: Molnar, 2005; Chanoine et al., 2005; Berkowitz et al., 2003
Conservative Interventions: Use of Weight Loss Drugs in Children • Weight loss achieved: mean difference of 2.61 kg weight change between placebo & control for orlistat (1-2 lbs/wk) • Pros: Consistent weight loss, little parental involvement, little behavioral change necessary • Cons: Long term safety has not been evaluated, side effects • Other drugs proposed, including metformin • Most pharmacologic regimes work best in combination with behavioral diet and physical activity changes Source: Molnar, 2005; Chanoine et al., 2005; Berkowitz et al., 2003; Freemark & Bursey, 2001
Drugs Currently Approved for Treatment of Obesity in Adults & Children in the U.S. * Approved for use in children in 2003 Source: Molnar, 2005
Drug Studies in Adolescents • Orlistat • Chanoine et al., JAMA 2005:293:2873-2883 • Multicenter, 54-week RCT, double blind, n = 539 obese adolescents, BMI > 2 units above 95th percentile, 12-16 years old • 120- mg dose of orlistat, plus mildly hypocaloric diet (30% kcal from fat), exercise, behavioral therapy • Results: • Difference in 0.86 BMI units (2.61 kg) • 35% attrition
Drug Studies in Adolescents • Sibutramine • Berkowitz et al., JAMA 2003;289:1805-1812 • RCT, double-blind (n = 82, 13-17 year olds, BMI = 32-44), 6 months, then open label for additional 6 months • Family-based behavioral program with sibutramine versus behavioral treatment • Difference of 4.6 kg between groups
Conclusions • There are limited data on obesity treatment and/or prevention studies conducted using preschool children. • Pharmacologic treatment has been evaluated on adolescents only (ages 12 and older). • Behavior modification programs that target diet and physical activity have been evaluated and are effective in children younger than 12, but need family involvement. • Increases in physical activity and decreases in sedentary activity are promising intervention strategies.
Conclusions • Children with extreme BMI/weight or have associated morbidity associated with overweight may need to engage in more aggressive interventions than those presented here. • Currently, conservative interventions are not complemented by a supportive environment for food availability and physical activity in most schools and communities.
Acknowledgements • Steve Kelder, MPH, PhD • Denny Bier, MD, PhD • William Klish, MD • Kristi King, MPH, RD • Tom Baranowski, PhD • Children’s Nutrition Research Center, Baylor College of Medicine, Houston, TX
Contact Information • Deanna M. Hoelscher, PhD, RD, LDAssociate ProfessorUniversity of Texas-Houston School of Public Health1200 Herman Pressler, RAS W942Houston, TX 77030713.500.9335713.500.9329 (fax)Deanna.M.Hoelscher@uth.tmc.edu • Website for SPAN survey: http://www.sph.uth.tmc.edu/hnc/SPANproject/SPAN%20Home.htm
References • Chanoine et al. Effect of orlistat on weight and body composition in obese adolescents. JAMA 2005;293:2873-2883. • Berkowitz et al., Behavior therapy and sibutramine for the treatment of adolescent obesity. JAMA 2003;289:1805-1812. • Freemark M & Bursey D. The effects of metformin on body mass index and glucose tolerance in obese adolescents with fasting hyperinsulinemia and a family history of type 2 diabetes. Pediatrics 2001;107:55.
References • Ebbeling et al. A reduced-glycemic load diet in the treatment of adolescent obesity. Arch Pediatr Adolesc Med 2003;157:773-779. • Spieth et al. A low-glycemic index diet in the treatment of pediatric obesity. Arch Pediatr Adolesc Med 2000;154:947-951. • Gutin et al., Effects of exercise intensity on cardiovascular fitness, total body composition, and visceral adiposity of obese adolescents. Am J Clin Nutr 2002;75:818-826.
References • Owens et al. Effect of physical training on total and visceral fat in obese children. Med Sci Sports Exercise 1999;31:143-148. • Kirk et al., Pediatric obesity epidemic: treatment options. J Am Diet Assoc. 2005;105:S44-S51. • Baker et al., Overweight children and adolescents: A clinical report of the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition. JPGN 2005;40:533-543. • Coates TJ & Thoresen CE. Treating obesity in children and adolescents: A review. Am J Public Health 1978:68:143-151.
References • Brown et al., A high protein, low calorie liquid diet in the treatment of very obese adolescents: long-term effect on lean body mass. Am J Clin Nutr 1983;38:20-31. • Stallings et al., One-year follow-up of weight, total body potassium, and total body nitrogen in obese adolescents treated wth the protein-sparing modified fast. Am J Clin Nutr. 1988;48:91-94. • Merritt et al. Consequences of modified fasting in obese pediatric and adolescent patients: effect of a carbohydrate-free diet on serum proteins. Am J Clin Nutr. 1981;34:2752-2755.
References • Butte N & Ellis K. Comment on “Obesity and the environment: Where do we go from here?” Science. 2003;301:598b. • Epstein et al. Ten-year follow-up of behavioral family-based treatment for obese children. JAMA 1990;264:2519-2523. • Epstein et al. Ten-year outcomes of behavioral family-based treatment for childhood obesity. Health Psychol. 1994;13:373-383. • Epstein et al., Treatment of pediatric obesity. Pediatrics. 1998;101:554-570.
References • Epstein et al., Do children lose and maintain weight easier than adults: A comparison of child and parent weight changes from six months to 10 years. Obesity Res. 1995;3:411-417. • Epstein LH & Squires S. The Stoplight Diet for Children. Toronto, CA: Little, Brown & Company, 1988. • Dietz WH. Overweight in childhood and adolescence. NEJM 2004;350:855-857
References • Molnar D. New drug policy in childhood obesity. Int J Obes 2005;29:S62-S65. • Kirschenbaum et al. The first significant weight losses during a follow-up period in an evaluation of weight loss camps for young people: Highly consistent self-monitoring at Wellspring Camps predicts even better long term results. Obes Res. 2005;13:A205.