Download
1 / 38
380 likes | 570 Vues
Developing a Coordinated Plan of Care. Partnership in End-of-Life Care. Donna S. Williamson, BSN, RNC, CHPN Palliative Care Consultant/LTC Facilitator Mountain Home, Arkansas. Objectives. Identify the benefits of developing a nursing facility/hospice partnership.

E N D
Developing a Coordinated Plan of Care Partnership in End-of-Life Care Donna S. Williamson, BSN, RNC, CHPN Palliative Care Consultant/LTC Facilitator Mountain Home, Arkansas
Objectives • Identify the benefits of developing a nursing facility/hospice partnership. • Assess whether care is being provided according to regulations. • Explain the steps in developing a coordinated care plan. • Identify the steps in implementing the care plan. • Identify problematic areas in developing a coordinated care plan.
Is Hospice Needed in the Nursing Home? What are your opinions of this NH staff? Hospice staff?
Hospice Needs the Nursing Facility When…. • Caregiver is inadequate • Caregiver is absent • Environment is unsafe • There is no provision in the Hospice Benefit for a primary caregiver. • The nursing facility can provide ‘room and board’
Nursing Facility Needs Hospice When…. • Physical symptoms are not controlled • Resident is in a non-skilled bed • Resident does not want to leave the facility • Resident does not want aggressive care • Psychosocial issues exist • Family in crisis • Other residents grieving • Facility staff grieving
The Federal Government Recognizes the Relationship “There is no indication in the statute that the term ‘home’ is to be limited for a hospice resident. A resident’s home is where he or she resides. The facility is considered to be the beneficiary’s place of resident (the same as a house or apartment), and the facility resident may elect the hospice benefit if he/she also meets the hospice eligibility criteria.” • Section 2082, State Operations Manual
Benefits of Partnership • Validation of care by an outside provider • CMS Quality Indicators are negative outcomes • Prevalent in the dying process • Two of the three sentinel events are common problems in the terminally ill resident. • Dehydration • Fecal impaction
Benefits of Partnership • Supporting Documentation • Hospice consent form: Resident elects to receive palliative care. • Physician terminal prognosis. • Advance directives. • Hospice team charting on quality indicators.
Benefits of Partnership • Hospice expertise • Symptom control • Psychosocial intervention • Spiritual care • Bereavement • Resident and family support • Dealing with ethical issues
Regulatory Basis • Nursing Facility Surveyor Guidelines • Hospice Guidelines • Fraud & Abuse Alert • Hospice Compliance Program
Hospice Admission Process • Resident elects hospice benefit • Hospice RN makes an initial visit performing complete assessment • Review physician orders to align with palliative care plan • Review assessment with MDS Coordinator and begin development of care plan • Sharing of Care plans • Joint care plan coordination • Document collaborative care planning
When the Resident Elects Hospice • They are either... • A new admission to the facility OR • A pre-existing resident
New Admission • Hospice must complete the assessment and care planning process within 48 hours upon admission. • Nursing facility has 21 days. • Hospice can share hospice problem list and care plan with MDS Coordinator.
Pre-Existing Resident • Nursing facility has completed MDS & Care Plan. • Complete a Significant Change in Condition form. • Prognosis of six months or less • Changed from acute to palliative care • No need to fill out future significant change forms as resident’s condition deteriorates • MDS triggers a new problem list • New care plan reflects palliative care
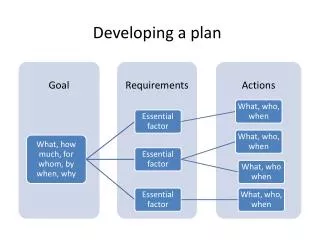
Determine Resident Problems • Develop a common problem list • All triggered problems do not require care planning • Problems may be identified that are not triggered
Determine Probable Outcomes • State Operations states: • “coordinated plan of care for both providers reflects hospice philosophy.” • Conditions of Participation for nursing facility states: • “the resident receives care and services to attain or maintain the highest practicable physical, mental and psychosocial well-being.” • Most Common source of tension and confusion in the relationship.
Hospice Outcomes • Self-Determined Life Closure • Anticipating death, mentally competent residents will have full autonomy to make decisions about how the remainder of their life is spent within the allowances of law. • Safe and Comfortable Dying • The resident will die free of distressing symptoms, in an environment that does not aggravate or hasten dying. • Effective Grieving • The expression of grief eventually supports the individual’s ability to adjust to their environment without the deceased & regain the ability to invest in other activities and relationships.
Nursing Facility Outcomes • After the comprehensive assessment process is completed, the interdisciplinary team will be able to decide if… • The resident has a troubling condition that warrants intervention, and addressing this problem is a necessary condition for other functional problems to be successfully addressed; • Improvement of the resident’s functioning in one or more areas is possible;
Nursing Facility Outcomes, cont. • Improvement is not likely, but the present level of functioning should be preserved as long as possible, with rates of decline minimized over time; • The resident is at risk of decline, and efforts should emphasize slowing or minimizing decline, and avoiding functional complications (e.g., contracture or pain) or; • The central issues of care revolve around symptom relief and other palliative measures during the last months of life.
Measuring Highest Practicable Functioning Resident Provision of Care Services Outcomes Negative Positive Avoidable Unavoidable
Determine Interventions • Reflect Hospice philosophy • Designate responsible provider • Designate responsible discipline • Establish when it will be done • Change and update to meet the resident’s needs
Area of Confusion in the Regulations • “Substantially all hospice core services (physician services, nursing services, medical social services, and counseling) must be routinely provided directly by hospice employees and cannot be delegated.” • “The hospice may involve the SNF/NF nursing personnel in assisting with the administration of prescribed therapies included in the plan of care only to the extent that the hospice would routinely utilize the services of a hospice resident’s family/caregiver in implementing the plan of care.”
Room and Board Services • Room and Board Services include: • Performing personal care service • Assisting with activities of daily living • Administering medication • Socializing activities • Maintaining cleanliness of a resident’s room • Supervising and assisting in the use of durable medical equipment and prescribed therapies
Hospice Prospective Payment • Requires the Professional Management of: • Services of the Interdisciplinary Team • Medication related to the terminal illness • Medical supplies related to the terminal illness • Durable medical equipment • Lab, x-ray, treatments, etc. • Inpatient care for periods of crisis • Resident does not have access to Medicare Part A services and has limited access to Part B services
Assessment and Care PlanningJust the Beginning… • Follow the steps of the nursing process • Remember…Outcomes are clinically “unavoidable” only if… • Accurately assessed • Adequate care is planned • The care plan is actually implemented • The interventions are evaluated periodically and modified according to the resident’s responses.
Nursing Facility SurveyorDeficiency on a Hospice Resident • Documentation in the MDS for Resident #2, noted the resident to have a short and long-term memory deficit and moderate impairment of cognitive function. • Record review identified the resident was being seen by a psychologist for individual therapy three times weekly for behaviors. • The resident was also being seen by a psychiatric consultant for management of her behaviors and antipsychotic medications. The resident is not cognitively aware to receive and participate in this therapy.
What’s Wrong with This Picture? • Resident #1 • This resident is obese and has congestive heart failure, cellulitis, edema, and stage-3 pressure ulcers. • According to the outcomes of the care plan, she has nothing to worry about because all these problems are going to be controlled or reversed.
What’s Wrong with This Picture? • Resident #2 – This resident is mentally retarded and has just undergone a colon resection for advanced colon cancer. • Problem: Alteration in thought process, impaired decision-making, impaired cognition secondary to diagnosis of mental retardation. • Goal: Resident will be able to make safe and reasonable decisions regarding care needs with the assistance of staff through next review • Intervention: Encourage resident to discuss reasons for inappropriate decisions and how they can be avoided in the future PRN.
What’s Wrong with This Picture? • Resident #3-This resident has cancer of the brain and is having seizures • Problem: Weight is above ideal weight. Family and resident are often non-compliant with diet. PO intake varies. • Goal: Resident will be free of weight gain from weight of 228 lbs. by next review. • Interventions: Sugar substitutes, skim milk with meals, encourage family to bring in healthier low-fat snacks.
What’s Wrong with This Picture? • Resident #4-The care plan reads: Notify hospice, without any other interventions for the hospice team. • Resident #5-This care plan has a hospice portion that is stapled to the nursing facility care plan. • Goal: Provide a safe and comfortable environment conducive to the death and dying process in which the physical, spiritual and psychosocial needs and symptoms will be addressed and resolved, and resident will die in a supportive, care-giving system in accordance with their wishes.
Who Are We Serving? • ? Regulator/Surveyor • ? Fiscal Intermediary • ? Nursing Facility • ? Resident • ? Family