Luteal Phase Deficiency in Female Reproductive Health
330 likes | 376 Vues
Explore definitions, causes, and pathophysiology of luteal phase deficiency, along with diagnosis and treatment options. Learn about how LPD affects infertility, pregnancies, and menstrual cycles.

Luteal Phase Deficiency in Female Reproductive Health
E N D
Presentation Transcript
Luteal phase deficiency Homamirzadapanah
outline • Definitions • Causes • Pathophysiology • Diagnosis • Treatment • Discussion
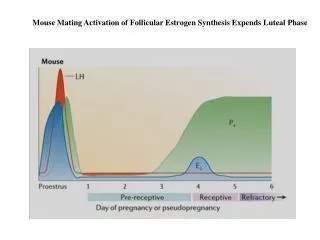
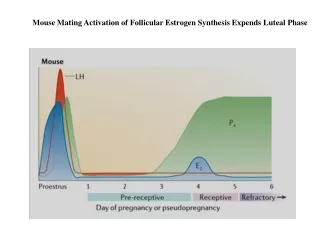
Luteal phase events are dependent on follicular recruitment and folliculogenesis
There is a shift of FSH dominance to LH dominance in luteal phase • Normal length of luteal phase in a non_fertile cycle is 14 days • After ovulation, luteinization of granulosa and theca cells occurs, progesterone is produced which maintains luteal phase
Theca cells derived from lutein cells are responsive to LH and produce progesterone in late luteal phase.
Definition • 1949, jones defined as corpus lutium defects in progesterone secretion • Luteal phase shorter than 12 days with relatively normal progesterone level • A normal length luteal phase with inadequate progesterone production or inadequate response of endometrium to normal progesterone production
4.4 % in fertile population • 3.5-13 % % in infertile patients • 13-32 % recurrent miscarriages
Luteal Phase Deficiency (LPD)Purportedly been associated with: • Infertility • 1st trimester pregnancy loss • Short cycles • Premenstrual spotting • Anorexia • Starvation • Eating disorders • Excessive exercise • Stress • Obesity & PCOS • Endometriosis • Aging • Thyroid dysfunction & hyperprolactinemia • Ovulation stimulation alone • Ovulation induction with or without GnRH agonists • ART
Causes • Abnormal folliculogenesis • Inadequate LH surge • Inadequate progesterone by corpus luteum • Aberrant and organ response by the endometrium
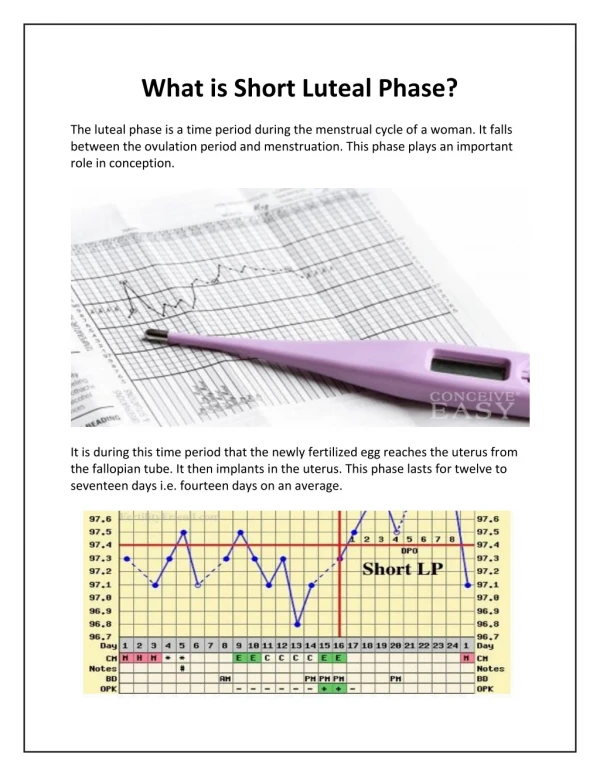
Short luteal phase • (LH peak ~ Onset of menstrual flow): Interval ≤ 8 days • 11–13 days Considered normal • Follicular phase abnormalities • Low follicular FSH levels • Altered follicular FSH/LH ratios • Abnormal FSH & LH pulsatility • ↓Luteal estrogen & progesterone levels • May occur in young healthy♀ with regular cycle length • Clinical consequences: unclear
pathophysiology • Follicular phase FSH has been implicated as a crucial factor in corpus luteum function • Other have focused on LH patterns secretion • An increased follicular LH frequency in follicular phase will leads to stunted luteal phase amplitude in luteal phase.
Clomiphene and LPD • Increase FSH to LH • Inadequate midcycle surge • Imbalance of estradiol to progesterone ratio • Anti estrogenic effect on endometrium
Gonadotropin and LPD • 30 % LPD • Stromal glandular dysfunction
Exercise and LPD • Prolong follicular phase • Strenuous exercise>4h/w
Recurrent spontaneous abortions • 32.5-60% • Horta and colleagues ; lower serum progesterone level in luteal phase in women with RPL • Babalioglu et all : endometrial biopsy and level of progesterone • 0
Diagnostic tests are influenced by and based upon the following physiologic observations: • Normal luteal phase length: 12–14 days • [Progesterone] peak in non-pregnancy cycles: 6 ~ 8 days after ovulation • Progesterone is secreted in pulses • Endometrial response: A reflection of the follicular phase estrogen & the luteal phase estrogen & progesterone
Methods proposed for diagnosing LPD • Basal body temperature (BBT) charting: • Inaccuracy, inconvenience, should be discouraged • Serum progesterone levels • Endometrial biopsy • Ovulation & adequate luteal length: • Urinary LH surge detection & Monitoring of luteal length
Progesterone Levels • Secreted in pulses (Reflect LH pulses) • Within 90 minutes: Fluctuate up to 8 fold • After ovulation (- pregnancy): peak 6 ~ 8 days • Determine peak progesterone levels • Need determine the time of ovulation • Urine LH false-positive LH surge
Endometrial Biopsy • Abnormalities of endometrial maturation: • Inadequate ovarian hormone secretion • Intrinsic endometrial abnormality • ‘‘Gold standard’’ to diagnose luteal inadequacy
Treatment approach to LPD • Treat two important cause of LP : Hyperprolactine or abnormal thyroid function • Clomiphene (CC) is not used as first line treatment modality for LPD as it can potentiality cause LPD
Treatment of potential luteal inadequacy • 1st approach: Correction of any underlying condition (hypothalamic or thyroid dysfunction, hyperprolactinemia) • 2nd: Empiric Treatment (based on limited reliable data) • Promote endometrial maturation • Enhance endometrial receptivity • Support implantation and development of an early pregnancy • Strategies: Progesterone, progesterone + estrogen, hCG in the luteal phase, Ovulation induction with clomiphene or gonadotropins
Progesterone supplementation • IM Progesterone Highest serum levels • Vaginal Progesterone ↑ Endometrial tissue levels • Oral progesterone • Only ~10% of micronized progesterone is absorbed intact through GI tract • ↓ Pregnancy rates • Should not be used for luteal support • Should be administered until placental progesterone production is adequate (8–10 weeks of gestation)
Conclusions • An adequate luteal phase is imperative for a pregnancy • Prevalence of LPD in natural cycles is 8% • however, the diagnosis remains difficult • The main hormone of he luteal phase is progesterone • LH is the main hormone, controlling he corpus Luteum • Rescue of the corpus Luteum: vaginal progesterone (7 weeks), but cave! 31 titel