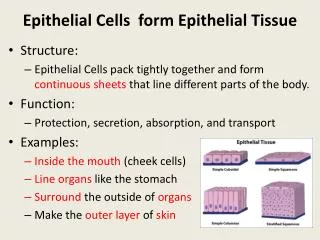
Junctional Epithelium / Epithelial Attachment
Junctional Epithelium / Epithelial Attachment. What and where it is Where it comes from What it does Why it does it. What and Where is the Junctional Epithelium. Epithelial attachment and clinical attachment level Collar-like band of nonkeratinised stratified squamous epithelium

Junctional Epithelium / Epithelial Attachment
E N D
Presentation Transcript
Junctional Epithelium / Epithelial Attachment What and where it is Where it comes from What it does Why it does it
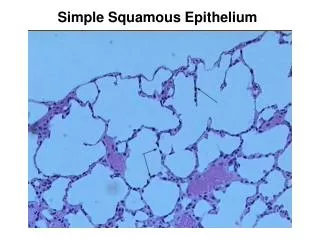
What and Where is the Junctional Epithelium • Epithelial attachment and clinical attachment level • Collar-like band of nonkeratinised stratified squamous epithelium • Extends from cementoenamel junction - bottom of gingival sulcus • Coronally: 15-30 cells thick. Apically: narrows to 1-3 cells • Length: 0.25 – 1.35mm & has rate of turnover
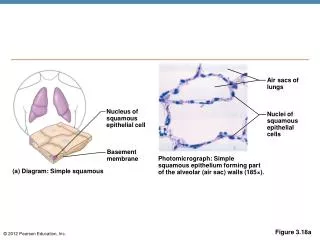
A- gingiva B- sulcular epithelium C- junctional epithelium D- lamina propria (connective tissue) E- alveolar process F- PDL ES- enamel space JE – junctional epithelium CT- connective tissue
Where does it come from ? • Initially derived from Reduced Enamel Epithelium • REE replaced once tooth erupts – REE covering crown lost rapidly replaced by squamous epithelial cells • Transformed REE & oral epithelium form dentogingival junction and junctional epithelium • Final conversion of REE to JE may not occur until 3-4 years post eruption
Important Features • Cells of JE immediately adjacent to tooth attach to tooth by hemidesmosomes & basal lamina • Combination is known as the epithelial attachment • Basal lamina in contact with tooth: Internal Basal lamina • On opposite surface – JE in contact with lamina propria of gingiva & attached by hemidesmosomes and basal lamina • Basal lamina in contact with lamina propria: External Basal Lamina
Junctional epithelium is unique as it possess 2 basement membranes – the internal and external basal lamina Enamel Lamina propria Hemidesmosomes Internal Basal Lamina External Basal Lamina
JE CT External basal lamina Enamel space Internal basal lamina
Enamel Cuticle • Not visible in demineralised sections • Non-mineralised structure between JE and underlying hard tissue • Cuticle also seen between JE and underlying cementum
Length of Junctional Epithelium • Length varies according to stage of eruption • Tooth first erupts – most of enamel covered by JE • Tooth reaches occlusal plane – ¼ enamel surface covered • Eventually JE lies close to CE junction • Older patients with root exposure (passive eruption or disease) JE proliferates apically - firm attachment with cementum
Other Fantastic Facts You Really Wanted to Know About the Junctional Epithelium!!!! • Lamina propria of gingiva – good vaculature and source of nutrient to JE and source of GCF • JE is permeable & tissue fluid and cells pass into GCF • Turnover of JE is rapid. Epithelial cells migrate coronally & shed into oral cavity via gingival crevice • Rate of turnover dependent on demands placed on tissue. Directly related to degree of inflammation
What it does and why it does it • Has attachment role and protective role • Permeability allows GCF and defence cells to pass across to protect underlying tissues from disease processes (periodonal disease) • Helps maintain integrity of tooth / periodontium structure.
Role of JE – Clincial significance • GCF contains g globulins and ploymorphonucleocytes (PNMs) giving it immunological / phagocytic properties to combat disease processes • Such molecules pass readily across JE to underlying tissues • JE (& GCF) good indicator for severity of periodontal disease – may contain neutrophils & other inflammatory cells indicating disease – & state of health of periodontium • Research into this ongoing in Bham – understanding progression of disease & development of diagnostic marker of severity of disease