Cease Smoking Today (CS2day) An Evidence-Based Approach To Treating Tobacco Dependence Focus on the Psychiatric Pat
Cease Smoking Today (CS2day) An Evidence-Based Approach To Treating Tobacco Dependence Focus on the Psychiatric Patient Scott M. Strayer, MD, MPH, FAAFP Associate Professor Departments of Family Medicine and Public Health Sciences University of Virginia Health System Question

Cease Smoking Today (CS2day) An Evidence-Based Approach To Treating Tobacco Dependence Focus on the Psychiatric Pat
E N D
Presentation Transcript
Cease Smoking Today (CS2day)An Evidence-Based Approach To Treating Tobacco DependenceFocus on the Psychiatric Patient Scott M. Strayer, MD, MPH, FAAFP Associate Professor Departments of Family Medicine and Public Health Sciences University of Virginia Health System
Question Which of the following statements regarding tobacco dependence and smoking cessation in patients with psychiatric disorders is/are correct?
Answers Rates of smoking are similar to individuals without psychiatric illness. Because of possible decompensation, smoking cessation is discouraged. Most psychiatric patients are highly motivated to quit smoking. Risks of most pharmacologic interventions outweigh the benefits. Smoking cessation may cause adverse reactions to psychiatric medications.
Smokers With Psychiatric Disorders Consume nearly ½ cigarettes smoked in US Spend nearly 40% of income on cigarettes Patients seeking tobacco dependence treatment 30 – 60% with past history of depression ≥ 20% with history of alcohol abuse or dependence Fiore MC, et al. U.S. DHHS Public Health Service 2008
Smokers With Psychiatric Disorders Chemical dependence > 70% smoke Increased mortality from tobacco-related diseases 1 study Fiore MC, et al. U.S. DHHS Public Health Service 2008
Smokers With Psychiatric Disorders May have greater sensitivity to nicotine dependence symptoms at lower levels of smoking Failing to address nicotine withdrawal may compromise psychiatric care for inpatients on smoke-free units. Fiore MC, et al. U.S. DHHS Public Health Service 2008
Answers Rates of smoking are similar to individuals without psychiatric illness. Because of possible decompensation, smoking cessation is discouraged. Most psychiatric patients are highly motivated to quit smoking. Risks of most pharmacologic interventions outweigh the benefits. Smoking cessation may cause adverse reactions to psychiatric medications.
Answers Rates of smoking are similar to individuals without psychiatric illness. Because of possible decompensation, smoking cessation is discouraged. Most psychiatric patients are highly motivated to quit smoking. Risks of most pharmacologic interventions outweigh the benefits. Smoking cessation may cause adverse reactions to psychiatric medications.
Outline • Assessment • 5 As • Interventions • Counseling • Pharmacotherapy
Case 22 yo Latino M, psychology student at local college, here for medication refill History of bipolar disorder Currently stable Several full blown episodes of mania and depression Hospitalized at age 19 during manic episode Depakote, Lithium
Case Past medical and surgical history Otherwise unremarkable Lives in an apartment with his girlfriend who smokes and a 2 year-old daughter
Case Smokes 1 pack/day cigarettes since 16 yo Recently increased to 2 packs/day Cope with stress at college Smokes when he drinks alcohol Wants to quit Unsure if he can Concerned about impact on bipolar disorder
Question At this time, all of he following interventions are recommended EXCEPT: Decrease cigarette intake by 25% every 1 to 2 weeks Initiate pharmacotherapy Follow-up with phone call 1 week after stopping Abstain from drinking beer Convince wife to stop smoking
Assessment of Tobacco Use Patient presents to a healthcare provider Does patient currently use tobacco? Yes No Is the patient currently willing to quit? Did the patient previously use tobacco? Yes No Yes No Provide appropriate treatments (5 As) Promote motivation to quit (5 Rs) Prevent relapse Encourage continuedabstinence
The 5 As For Patients Willing to Quit • ASK about tobacco use • ADVISE to quit • ASSESS willingness to make a quit attempt • ASSIST in quit attempt • ARRANGE for follow-up Fiore MC, et al. U.S. DHHS Public Health Service 2008
Ask • 70% of smokers want to quit • 81% have tried to quit at least once • Only 7 to 15% very reluctant to discuss quitting smoking • EVERY patient at EVERY visit Fiore MC, et al. U.S. DHHS Public Health Service 2008
Vital Signs Stamp VITAL SIGNS Blood Pressure: Pulse: Weight: Temperature: Respiratory Rate: Tobacco Use: Current Former Never (circle one) Fiore MC, et al. U.S. DHHS Public Health Service 2008
Advise • Advice should be clear, strong and personalized. Fiore MC, et al. U.S. DHHS Public Health Service 2008
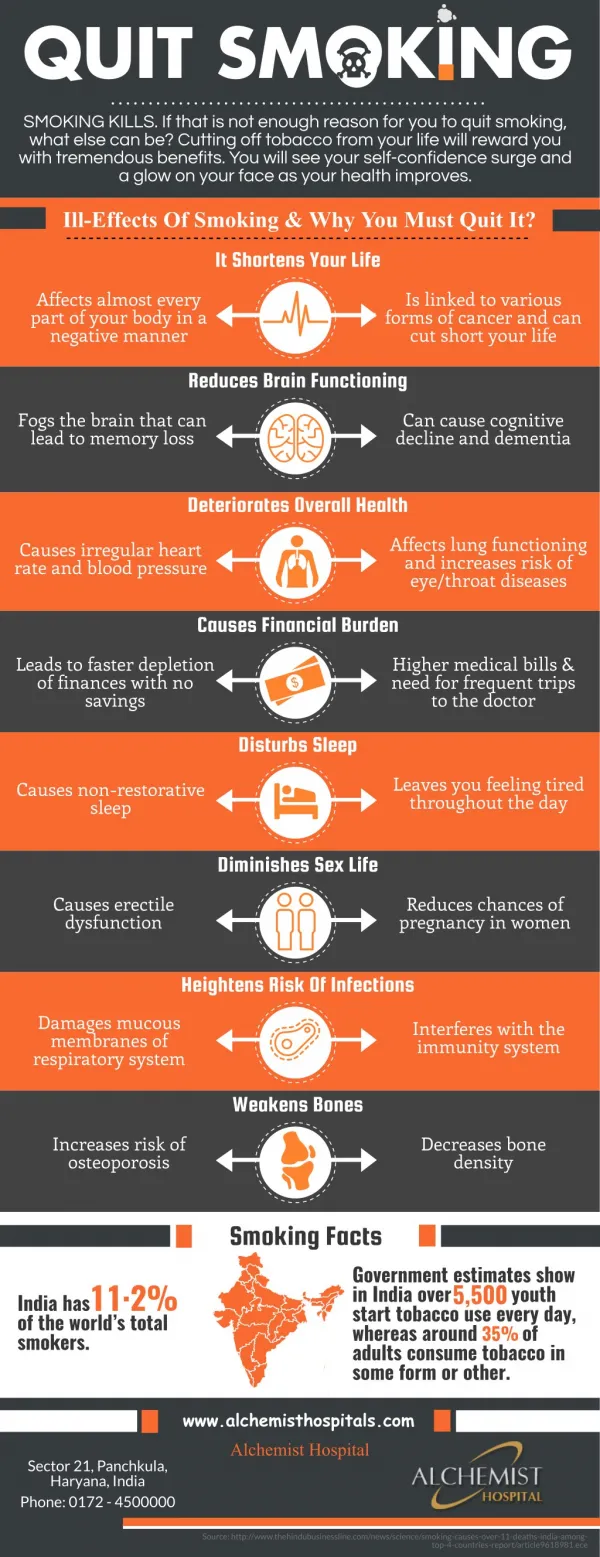
Advise • 37.5% of preventable causes of death are tobacco-related • 1/3 of all tobacco users will have a decreased life span • 13.2 years in men • 14.5 years in women • Someone dies from tobacco use every 8 seconds Fiore MC, et al. U.S. DHHS Public Health Service 2008
AdviseSmokers With Psychiatric Disorders Chemical dependence Increased mortality from tobacco-related diseases versus other patient populations 1 study Fiore MC, et al. U.S. DHHS Public Health Service 2008
Advise • Never too late to quit • Age 40: gain 9 years • Age 50: gain 6 years • Age 60: gain 3 years Fiore MC, et al. U.S. DHHS Public Health Service 2008
Assist • S et a quit date to stop completely • Ideally within 2 weeks • T ell family & friends • A nticipate challenges • R emove tobacco products from environment (home, work, car) Fiore MC, et al. U.S. DHHS Public Health Service 2008
AssistTriggers & Challenges Where, when, why does patient smoke Alcohol Other smokers “Urges” and “Cues” Withdrawal symptoms Prior quit experience Build on success Fiore MC, et al. U.S. DHHS Public Health Service 2008
AssistTriggers & Challenges Concern about weight gain Negative affect, stressors Mental illness Increased risk of relapse Lack of support Lack of self efficacy Lack of knowledge Fiore MC, et al. U.S. DHHS Public Health Service 2008
Assist • Counseling & behavioral therapies • Pharmacotherapy Fiore MC, et al. U.S. DHHS Public Health Service 2008
AssistSmokers With Psychiatric Disorders Smoking cessation and/or nicotine withdrawal may exacerbate underlying psychiatric condition. Consider waiting until psychiatric symptoms stabilized before initiating smoking cessation interventions. Case by case basis Fiore MC, et al. U.S. DHHS Public Health Service 2008
Arrange Relapse Most likely within 1st 3 months Especially 1st 2 weeks Recommended follow-up Ideally within 1st week after quitting 2nd contact within 1st month Further follow-up based on need Fiore MC, et al. U.S. DHHS Public Health Service 2008
ArrangeSmokers With Psychiatric Disorders Increased risk of relapse Fiore MC, et al. U.S. DHHS Public Health Service 2008
Askabout tobacco use. Adviseto quit. Assesswillingness to make a quit attempt. Assistin quit attempt.For patients unwilling to quit at the time, provide motivational interventions designed to increase future quit attempts. Arrangefollow-up.For patients unwilling to make a quit attempt at the time, address tobacco dependence and willingness to quit at next clinic visit. The “5 As” Model – 2008 Update Fiore MC, et al. U.S. DHHS Public Health Service 2008
Question At this time, all of he following interventions are recommended EXCEPT: Decrease cigarette intake by 25% every 1 to 2 weeks Initiate pharmacotherapy Follow-up with phone call 1 week after stopping Abstain from drinking beer Convince wife to stop smoking
Question At this time, all of he following interventions are recommended EXCEPT: Decrease cigarette intake by 25% every 1 to 2 weeks Initiate pharmacotherapy Follow-up with phone call 1 week after stopping Abstain from drinking beer Convince wife to stop smoking
Question Of the following statements regarding the non-pharmacologic treatment of this patient’s tobacco dependence, which is correct?
Answers Quit lines alone are effective in achieving abstinence. The addition of counseling to medications does not increase abstinence rates. Physicians are much more effective than non-physician clinicians at delivering treatment. Individual counseling alone is ineffective in achieving abstinence. Teaching problem solving and skills training alone is ineffective in achieving abstinence.
Counseling Strong dose-response relationship Fiore MC, et al. U.S. DHHS Public Health Service 2008
CounselingIntensity of Clinical Interventions Fiore MC, et al. U.S. DHHS Public Health Service 2000. Meta-analysis (n = 43 studies).
Estimating Likelihood of Abstinence Fiore MC, et al. U.S. DHHS Public Health Service 2008
Smokers With Psychiatric Disorders May have greater sensitivity to nicotine dependence symptoms at lower levels of smoking Increased risk of relapse Fiore MC, et al. U.S. DHHS Public Health Service 2008
CounselingComponents of Intensive Treatment Population Program clinicians Program intensity Program format Type of counseling and behavioral therapies Medication Fiore MC, et al. U.S. DHHS Public Health Service 2008
CounselingComponents of Intensive Treatment Population All tobacco users willing to participate in such efforts Optimizes likelihood of abstinence Fiore MC, et al. U.S. DHHS Public Health Service 2008
CounselingComponents of Intensive Treatment Program clinicians Physicians and non-physician clinicians equally effective 2 clinician types optimal Fiore MC, et al. U.S. DHHS Public Health Service 2008
CounselingComponents of Intensive Treatment One counseling strategy Physician Delivers strong message to quit Discusses health benefits of quitting Prescribes medications Non-physician clinician Delivers additional counseling & behavioral interventions Fiore MC, et al. U.S. DHHS Public Health Service 2008
CounselingComponents of Intensive Treatment Program intensity Session length > 10 minutes Number of sessions ≥ 4 sessions Total contact time 30 – 90 minutes Fiore MC, et al. U.S. DHHS Public Health Service 2008
CounselingComponents of Intensive Treatment Program format Effective Individual or group counseling Proactive telephone counseling, including Quit lines 1 – 800 – QUIT – NOW Fiore MC, et al. U.S. DHHS Public Health Service 2008
CounselingComponents of Intensive Treatment Program format Optional Self help materials and cessation Web sites Multiple formats optimal, with use of 3 – 4 types especially effective Fiore MC, et al. U.S. DHHS Public Health Service 2008
Type of counseling & behavioral therapy Practical counseling Problem solving/skills training/stress management Intra-treatment social support Direct contact with clinician CounselingComponents of Intensive Treatment Fiore MC, et al. U.S. DHHS Public Health Service 2008
Types of counseling & behavioral therapies recommended by 2000 but not 2008 guideline Extra-treatment social support Smoker’s environment Aversive smoking procedures Rapid smoking, rapid puffing, other smoking exposure CounselingComponents of Intensive Treatment Fiore MC, et al. U.S. DHHS Public Health Service 2008
Practical Counseling Problem Solving/Skills Training Fiore MC, et al. U.S. DHHS Public Health Service 2008
Counseling Intra-treatment Supportive Treatment Fiore MC, et al. U.S. DHHS Public Health Service 2008
Combination of Counseling and Medication Superior to Either Treatment Alone Fiore MC, et al. DHHS Public Health Service 2008. Meta-analysis, Combination vs medication alone (n = 18 studies) and vs counseling alone (n = 9 studies).