Download
1 / 33
350 likes | 755 Vues
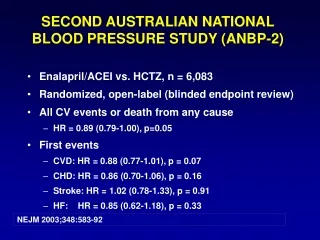
Second Australian National Blood Pressure Study. ANBP 2. Conducted by the High Blood Pressure Research Council of Australia in conjunction with Australia’s General Practitioners. Background. Treatment of hypertension based on diuretics and/or beta blockers provides a definite outcome benefit

E N D
Second Australian National Blood Pressure Study ANBP2 Conducted by the High Blood Pressure Research Council of Australia in conjunction with Australia’s General Practitioners
Background • Treatment of hypertension based on diuretics and/or beta blockers provides a definite outcome benefit • Additional benefit beyond that resulting from blood pressure reduction may result with therapy based on agents inhibiting the renin-angiotensin system ANBP2 New Engl J Med, 2003;348:583-92.
ANBP2 Background • No outcome data with ACE inhibitor based regimens • Potential benefits include • Reduction in LVH • Improved survival with cardiac failure • Enhanced insulin sensitivity • Lipid “neutrality” Will outcome be the same better or worse than those of published studies?
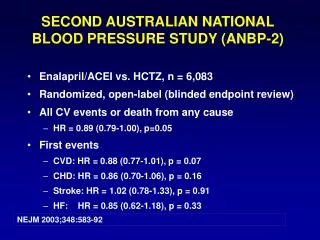
Main Aim To determine in hypertensive patients aged 65-84 years whether there is any difference in total cardiovascular events (fatal and non-fatal) over a 5 year treatment period between treatment with either a diuretic-based regimen or an ACE inhibitor-based regimen ANBP2 New Engl J Med, 2003;348:583-92.
Pprospective Rrandomised Oopen label Bblinded Eendpoints Features Intention to treat General practice based 600 practices 6000 patients Recruitment: 2.5 years Study Design ANBP2 New Engl J Med, 2003;348:583-92.
Management Committee (HBPRCA) Sub Committees General Practice Data monitoring End - point Audit Substudies: ABPM, LVH, Genetic, Health Econ National Centre (BMRI) Regional Centers SA QLD VIC NSW WA Data Management Centre (Uni of Adelaide) Study Organisation ANBP2
Study Subjects Inclusion Criteria • Men and women 65 - 84 years • Previously treated or newly diagnosed hypertensives • Untreated sitting SBP> 160 and/or DBP >90 mmHg • Able to give consent and to attend GP practice • No recent cardiovascular morbidity Exclusion Criteria • Any cardiovascular end-point in the past 6 months • Dementia • Plasma creatinine > 0.2 mmol/L • Any life threatening illness (unlikely to survive 5 years) • Unwillingness of GP to enter subject into study • Unable to attend GP practice • Absolute contraindication to ACE or diuretic ANBP2 New Engl J Med, 2003;348:583-92.
ANBP2 Study Protocol • Blood Pressure Screening • 3 visits conducted by Study Nurses • 3 measurements (average of 2nd and 3rd) • Mercury sphygmomanometer • Entry BP - average of 2nd and 3rd visit readings • Randomisation • Central - Data Management Centre (Adelaide) • Stratified for age (> or 75) • Follow-Up • GP manages patient according to usual practice • Conform (where possible) to randomisation arm • Achieve subject goal BP • At least 2 visits per year New Engl J Med, 2003;348:583-92.
ANBP2 Study Drug Treatments • ACE Inhibitor Group • Step 1. ACE Inhibitor (enalapril recommended) • Step 2. Beta or alpha blocker or calcium antagonist • Step 3. Drug from class not used in Step 2 or diuretic • Step 4. Drug from class not used in step 2 or 3 • Diuretic Group • Step 1. Thiazide type diuretic (low dose) • Step 2. Beta or alpha blocker or calcium antagonist • Step 3. Drug from class not used in Step 2 • Step 4. Drug from class not used in step 2 or 3 New Engl J Med, 2003;348:583-92.
Study End-points • Obtained by study nurses from GP case notes, hospital case records and death certificates • End-point Committee (blinded to treatment allocation) evaluated all data relating to potential study end-points • Primary Outcome: All cardiovascular events (initial and subsequent) or death from any cause – ‘total burden of cardiovascular disease’ • Any first eventor death – ‘event-free survival’ • Cause-specific first events ANBP2 New Engl J Med, 2003;348:583-92.
End-points • myocardial infarction (fatal and non-fatal) • sudden or rapid or ‘other’ cardiac death • coronary events resulting in coronary therapeutic procedures • cardiac failure (fatal or non-fatal) • stroke (fatal or non-fatal) • transient cerebral ischaemic attacks • acute non-coronary or non-cerebral vascular occlusion • other vascular deaths • dissecting or ruptured aortic aneurysm ANBP2 New Engl J Med, 2003;348:583-92.
Data Analysis • Multivariate proportional hazards (Cox) models incorporating: • Wei-Lin-Weissfeld method for multiple failure time data • Li-Lagakos application of WLW method to analyse recurrent event data with a terminating event • Robust variance estimation • Validation by simulation • Proportional hazards (Cox) models for cause-specific first events ANBP2 New Engl J Med, 2003;348:583-92.
ANBP2 GP Involvement in ANBP2 2681 - GPs 1594 - Practices 500 299 472 224 361 200 390 270 958 601 New Engl J Med, 2003;348:583-92.
7530 849 11% 7448 763 10% 14669 1310 9% 7607 672 9% 17145 2489 15% ANBP2 ANBP2 Subject Recruitment Screened - 54288 Randomised - 6083 Rate - 11%
Study profile 54288 screened 25805 ineligible 16899 unwilling to participate 5501 did not meet inclusion criteria ~ 3 yrs 6083 randomised ACE 3044 Diuretic 3039 ITT* analysis Observation Time Median 4.1 yrs Patient yrs 24702 0 No Vital Status 2 ACE 3044 Diuretic 3037 ANBP2 * Intention to treat New Engl J Med, 2003;348:583-92.
Baseline data ACE Diuretic (3044) (3039) Male: Female 50:50 48:52 Age (yr) 72.0 71.9 Blood Pressure (mmHg) 167 ± 13 168 ± 13 91 ± 8 91 ± 8 Previously Treated 62% 62% Body Mass Index (kg/m2) 27 ± 4 27 ± 4 Current Smokers 7% 7% Physically Active 78% 76% ANBP2 New Engl J Med, 2003;348:583-92.
Baseline data ACE Diuretic (3044) (3039) Coronary Heart Disease 8% 8% Cerebrovascular Disease 5% 5% Diabetes Mellitus 8% 7% Hypercholesterolaemia 38% 36% - lipid lowering drugs 13% 13% ANBP2 New Engl J Med, 2003;348:583-92.
Drug treatments At Randomisation At Study End ACE Diuretic ACE Diuretic (3044) (3039) (3044) (3039) Allocated Therapy 83% 83% 58% 62% Monotherapy 82% 82% 65% 67% 3 agents 6% 5% No drugs 16% 15% 4% 3% ANBP2 New Engl J Med, 2003;348:583-92.
Antihypertensive Medication Use at Study End ACE Diuretic ACE 58 18 Beta Blocker 11 14 Ca Blocker 23 25 Diuretic 24 62 Single Drug 65 67 2 Drugs 25 25 3 + Drugs 6 5 Data represent % ANBP2 New Engl J Med, 2003;348:583-92.
In-study blood pressure -26 mmHg -12 mmHg ANBP2 New Engl J Med, 2003;348:583-92.
Primary Result ACE Diuretic Event n Rate n Rate HR (95%CI) p All cardiovascular 692 55.8 732 59.5 0.89 (0.79,1.00) 0.05 events or any death First cardiovascular 490 41.9 529 45.7 0.89 (0.79,1.01) 0.06 event or death Death 195 15.7 210 17.1 0.90 (0.75,1.09) 0.27 Rate per 1000 patient years Adjusted for age, gender ANBP2 New Engl J Med, 2003;348:583-92.
Primary Result Rate per 1000 patient years Adjusted for age, gender ANBP2
Cause-specific first events All subjects - first any events ANBP2 New Engl J Med, 2003;348:583-92.
Cause-specific fatal events All subjects - fatal events ANBP2 New Engl J Med, 2003;348:583-92.
Cause-specific non-fatal events All subjects - first non-fatal events ANBP2 New Engl J Med, 2003;348:583-92.
Summary • 11% reduction in total cardiovascular events (or death from any cause) with ACE inhibitor treatment • 11% reduction in first events with ACE inhibitor treatment • 17% reduction in total events in males and no effect in females ANBP2 New Engl J Med, 2003;348:583-92.
Summary • No difference between treatments • total or cardiovascular mortality • all cerebrovascular events • all coronary events • With ACE inhibitor treatment • reduction in first non-fatal cardiovascular events (HR 0.86) • reduction in non-fatal myocardial infarctions (HR 0.68) • increase in fatal strokes (HR 1.91) • cause-specific effects only in males ANBP2 New Engl J Med, 2003;348:583-92.
Conclusion Initiation of antihypertensive treatment in older patients with an ACE inhibitor particularly in males has a modest but definite outcome advantage over a diuretic despite a similar reduction in blood pressure ANBP2 New Engl J Med, 2003;348:583-92.
Acknowledgments • Australian Commonwealth Department of Health and Ageing • National Health and Medical Research Council of Australia • Study staff • Australia’s General Practitioners • Merck Sharp & Dohme (Australia) Pty Ltd ANBP2
Acknowledgments Prof L. Wing (SA - Chairperson) Dr C. Reid (Vic - Study Director) Dr P. Ryan (SA - Statistician) Prof G. Jennings (Vic) Prof J. McNeil (Vic) Prof M. Brown (NSW) Prof C. Johnston (Vic) Prof T. Morgan ( Vic) Prof J. Marley (SA) Prof L. Beilin (WA) Prof M. West (Qld) Prof G. MacDonald (NSW) ANBP2 Management Committee ANBP2
Acknowledgments Regional Co-ordinating Centres: Mark Nelson, Anne Bruce, Paul Beckinsale, Jill Thompson, Marilyn McMurchie, Glenda Fraser, David Gleave, Vicki Cope, Fred DeLooze, Sue Moore, Cathy Dibben, Jonathon Newbury Data Management and National Coordinating Centres: Helen Miles, Brian McDermott, Kristyn Willson, Carol Bear Genetic Sub-Committee: Malcolm West, Stephen Harrap, Colin Johnston, Lawrie Beilin, Philip Ryan, Lindon Wing, Christopher Reid Ambulatory Blood Pressure Monitoring Sub-Committee: Lawrie Beilin, Mark Brown, Philip Ryan, Lindon Wing, Christopher Reid LVH Sub-Committee: Garry Jennings, Peter Fletcher, Michael Feneley, Elizabeth Dewar, Lindon Wing, Christopher Reid ANBP2
Acknowledgments Data Audit Sub-Committee: John McNeil, Lindon Wing, John Marley, Christopher Reid Finance Sub-Committee: Colin Johnston, Garry Jennings, Lindon Wing, Christopher Reid Health Economic/Quality of Life Sub-Committee: John Marley, John Moss, Penny Webb, Paul Glasziou, Fran Boyle, John Primrose, Lindon Wing, Christopher Reid GP Advisory Committee: Ian Steven, Leon Piterman, Fred De Looze, Jim Dickinson, John Gambrill, Peter Joseph, Christopher Reid End-point Committee:David Hunt, Geoff Donnan, Lindon Wing, Trefor Morgan Independent Data Audit Sub-Committee: John Chalmers, Judith Whitworth, Stephen MacMahon, Chris Silagy (Decd) ANBP2