Download
1 / 1
10 likes | 140 Vues
Discussion. References:. Introduction. Clinical Course. Eosinophilic Pulmonary Infiltrates In A Child Infested With Giardia Lamblia – An Association Or Coincidence? J. Schwarz, DO; J. Kim, MD; E. Rosenfeld, MD; M. Tsifansky, MD.

E N D
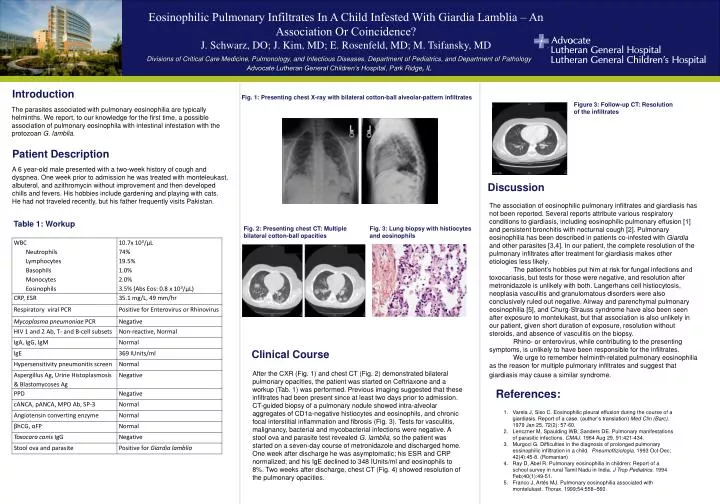
Discussion References: Introduction Clinical Course • Eosinophilic Pulmonary Infiltrates In A Child Infested With Giardia Lamblia – An Association Or Coincidence? J. Schwarz, DO; J. Kim, MD; E. Rosenfeld, MD; M. Tsifansky, MD Divisions of Critical Care Medicine, Pulmonology, and Infectious Diseases, Department of Pediatrics, and Department of Pathology Advocate Lutheran General Children’s Hospital, Park Ridge, IL Fig. 1: Presenting chest X-ray with bilateral cotton-ball alveolar-pattern infiltrates Figure 3: Follow-up CT: Resolution of the infiltrates The parasites associated with pulmonary eosinophilia are typically helminths. We report, to our knowledge for the first time, a possible association of pulmonary eosinophila with intestinal infestation with the protozoan G. lamblia. Patient Description A 6 year-old male presented with a two-week history of cough and dyspnea. One week prior to admission he was treated with monteleukast, albuterol, and azithromycin without improvement and then developed chills and fevers. His hobbies include gardening and playing with cats. He had not traveled recently, but his father frequently visits Pakistan. The association of eosinophilic pulmonary infiltrates and giardiasis has not been reported. Several reports attribute various respiratory conditions to giardiasis, including eosinophilic pulmonary effusion [1] and persistent bronchitis with nocturnal cough [2]. Pulmonary eosinophilia has been described in patients co-infested with Giardia and other parasites [3,4]. In our patient, the complete resolution of the pulmonary infiltrates after treatment for giardiasis makes other etiologies less likely. The patient’s hobbies put him at risk for fungal infections and toxocariasis, but tests for those were negative, and resolution after metronidazole is unlikely with both. Langerhans cell histiocytosis, neoplasiavasculitis and granulomatous disorders were also conclusively ruled out negative. Airway and parenchymal pulmonary eosinophilia [5], and Churg-Strauss syndrome have also been seen after exposure to montelukast, but that association is also unlikely in our patient, given short duration of exposure, resolution without steroids, and absence of vasculitis on the biopsy. Rhino- or enterovirus, while contributing to the presenting symptoms, is unlikely to have been responsible for the infiltrates. We urge to remember helminth-related pulmonary eosinophilia as the reason for multiple pulmonary infiltrates and suggest that giardiasis may cause a similar syndrome. Table 1: Workup Fig. 2: Presenting chest CT: Multiple bilateral cotton-ball opacities Fig. 3: Lung biopsy with histiocytes and eosinophils After the CXR (Fig. 1) and chest CT (Fig. 2) demonstrated bilateral pulmonary opacities, the patient was started on Ceftriaxone and aworkup (Tab. 1) was performed. Previous imaging suggested that these infiltrates had been present since at least two days prior to admission. CT-guided biopsy of a pulmonary nodule showed intra-alveolar aggregates of CD1a-negative histiocytes and eosinophils, and chronic focal interstitial inflammation and fibrosis (Fig. 3). Tests for vasculitis, malignancy, bacterial and mycobacterial infections were negative. A stool ova and parasite test revealed G. lamblia, so the patient was started on a seven-day course of metronidazole and discharged home. One week after discharge he was asymptomatic; his ESR and CRP normalized; and his IgE declined to 348 IUnits/ml and eosinophils to 8%. Two weeks after discharge, chest CT (Fig. 4) showed resolution of the pulmonary opacities. Varela J, Siso C. Eosinophilic pleural effusion during the course of a giardiasis. Report of a case. (author’s translation) Med Clin (Barc). 1979 Jan 25, 72(2): 57-60. Lenczner M, Spaulding WB, Sanders DE. Pulmonary manifestations of parasitic infections. CMAJ. 1964 Aug 29, 91:421-434. Murgoci G. Difficulties in the diagnosis of prolonged pulmonary eosinophilic infiltration in a child. Pneumoftiziologia. 1993 Oct-Dec; 42(4):45-8. (Romanian) Ray D, Abel R. Pulmonary eosinophilia in children: Report of a school survey in rural Tamil Nadu in India. J Trop Pediatrics. 1994 Feb;40(1):49-51. Franco J, Artés MJ. Pulmonary eosinophilia associated with montelukast. Thorax. 1999;54:558–560.






