Download
1 / 79
990 likes | 1.73k Vues
Surgical Management Of Medically Intractable Temporal Lobe Epilepsy. By Amr Farid Lecturer Of Neurosurgery Mansoura University. Why we should help?. Quality of life Physical injury Neuropsychological functions impairment Psychiatric problems Sudden unexpected death in epilepsy

E N D
Surgical Management Of Medically Intractable Temporal Lobe Epilepsy By AmrFarid Lecturer Of Neurosurgery Mansoura University
Why we should help? • Quality of life • Physical injury • Neuropsychological functions impairment • Psychiatric problems • Sudden unexpected death in epilepsy • Complications of AEDs (Inexperienced prescriptions)
Introduction • Seizure classification: • 1. Partial seizures • A) Simple partial seizure • Motor • Sensory • Autonomic • Psychic • B) Complex partial • With simple partial onset • Without simple partial onset, altered awareness / memoryfrom the onset • C) Partial seizures (simple or complex) evolving to secondary generalization
Introduction • 2. Primary generalized (convulsive or nonconvulsive) • Absence seizures. • Myoclonic seizure • Clonic , tonic and tonic-clonic seizures • Atonic seizures • 3. Unclassified seizures • 4. Prolonged or repetitive seizures (status epilepticus)
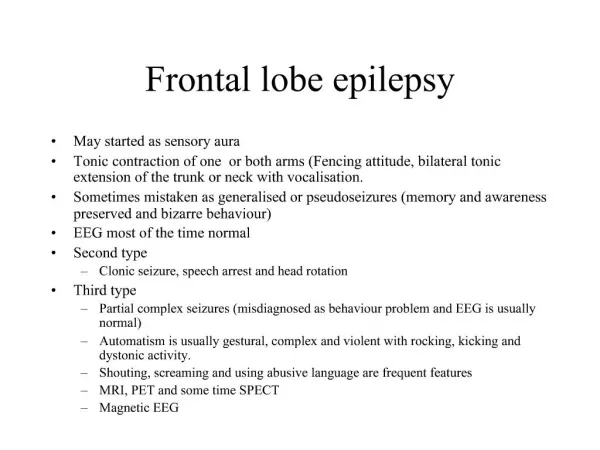
Introduction Introduction Mesial and Neocortical Temporal Epilepsy Clinical Features MTLE NTLE A phenomenon of dreamy state with memory of past scenes (déjà vu ) Auditory hallucinations Early contralateraldystonic posturing. Rapid spread to suprasylvian area produce versive and colonic motor movement of head ,eye and face. • Warning symptoms localized to the epigastrium ,throught, or chest with or without fear. • Initial motionless staring • oro-alimentary masticatory or swallowing automatisms with or without repetitive manual automatism • Seizures are significantly longer in duration (> 1 minute). • Ipsilateral automatisms followed by contralateraldystonic posturing.
Introduction Localization of Partial Seizure Focus 20% 10% 70% • This is the most common type of adult-onset epilepsy. • Causes such as hippocampal sclerosis, low- grade tumors and cortical dysplasias , vascular malformation
Introduction • Pre-operative Assessment • Electro physiologically • Electroencephalography (EEG) • Continuous Video EEG • Value OF EEG • Diagnostic tool • Spikes , poly spike • Sharp wave • Sharp and slow waves • complexes.
Introduction • Limitations of EEG: • Normal EEG findings do not exclude epilepsy. • The initial EEG may show normal results in 50% of cases. • Increasing the duration of recording. • Deep focus. • Artifact
Introduction • Electrode Placement • (A) Non invasive electrodes • 1- Scalp Electrodes: • Standard 10-20 system. • 2- Zygomatic and Periorbital Electrodes: (Anterior temporal foci)
Introduction The international 10-20 electrode system
Introduction • (B) Semi-invasive Electrodes • Nasopharyngeal Electrodes: mesialtemporal and orbitofrontal foci. • Sphenoidal Electrodes: for long term ,with less artifacts. • Foramen Ovale Electrodes: mesiobasal temporal lobe epilepsy. • Tympanic Electrodes: middle or posterior basal temporal regions
Introduction • (C) Invasive Electrodes • Epidural Electrodes • Subdural Strip and Grid Electrodes • Implanted Intracerebral Electrodes (Depth Electrodes) • Seizures are lateralized but not localized (eg, a left-sided). • Seizures are localized but not lateralized (eg, both temporal lobes). • Seizures are neither localized nor lateralized (eg. diffuse ictal). • Seizure localization is discordant with other data • Intraoperative , ECoG
Introduction Partial Onset Seizure – Left TLE Generalized Onset Seizure
Introduction Generalized Focal to generalized Focal Origin Of EEG abnormality
Introduction • Neuroradiology • Functional Magnetic Resonance Imaging (fMRI): • PET and SPECT imaging especially has shown both increased glucose metabolism and blood flow respectively in the epileptic cortex, which is depressed in the post-ictal and interictal states. • MRS is a newer tool that demonstrates regional metabolic alteration in epileptogenic tissue. • Magnetoencephalography: • Measurement of extracranial magnetic fields
Introduction Cutting planes Imaging issues: strategies for successful interpretation • (HIPPO SAGE)
Introduction MRI features of HS • Secondary signs • Unilateral atrophy of the mamillary body, fornix ,amygdala. • Increased T2 W signal in ant. temporal • white matter with loss of grey-white demarcation in the ipsilateral anterior temporal lobe. • Unilateral dilatation of the temp. horn. • Primary signs • Atrophic unilateral hippocampus . • Hyperintensity on both T2 W and FLAIR images • Loss of the hippocampal internal architecture and that of normal digitations of the head.
Introduction Functional and Morphologic Data Fusion for Epileptogenic Foci Localisation MRI +SPECT (Lt TLE) MRI-PET fusion image (Lt TLE)
Introduction Scheme for preoperative evaluation in TLE
Introduction • Surgical Treatment of TLE • General Surgical procedures: • Resection techniques is simple excision of the structural lesion • Disconnection techniques (hippocampaltransection ) • Augmentation techniques ( vagal stimulation). • Gamma knife radiosurgery • Stereotactic radiofrequency ablation techniques .
Introduction Epileptic Zones
Introduction • Temporal Lobectomy: • Temporal lobe resection produces a seizure-free state in 60% to 80 % of patients: • Anterior temporal lobectomy (ATL) is the most common surgical procedure performed in adolescents and adults. • Selective Amygdalohippocampectomy for patients with MTLE
Introduction Temporal Lobectomy: A) Anterior temporal lobectomy with amygdalo-hippocampectomy
Introduction B) Selective Approaches to The Mesial Temporal Area
Introduction Trans-sylvian approach
Introduction Meyer’s loop • Risk for superior quadrant hemianopsia • 50 –100% after standard temporal lobectomy • up to 50% after trans-sylvian selective amygdalohippocampectomy
Aim Of The Work
This study is to compare: • seizure and neuropsychological outcomes after: • Anterior temporal lobe resection plus amygdalo-hippocampectomy (AH) • versus selective amygdalo-hippocampectomy (AH) through trans sylvian approach • In the treatment of medically intractable temporal lobe epilepsy
Patients & Methods
Patients & Methods This study was conducted on 24 patients with medically intractable Temporal Lobe Epilepsy at Tohoku University Hospital.
Patients & Methods • Inclusion criteria • Medically intractable epilepsy due to identified temporal lobe focus. • Lesions may be intra or extra axial within the anatomical confines of the temporal lobe. • Both of neocortical and mesial temporal lobe. • Exclusion criteria • Patients unfit for surgery. • Presence of multiple brain lesions. • Pure extratemporalepileptogenic zone.
Patients & Methods • Presurgical evaluation • Drug resistant epilepsy : failure of two tolerated, appropriately chosen (whether as monotherapies or in combination) to achieve sustained seizure freedom over period of two years. • Detailed history :patients and close contact. • Clinical assessment • Electrophysiological assessment via ( VEEG). • Neuroimaging via routine MRI brain ,(FDG-PET), Interictal SPECT and magneto-encephalography (MEG) were done to confirm diagnosis.
Patients & Methods Neuropsychological Test Battery • Wechsler Adult Intelligence scale (WAIS-R: VIQ, PIQ, FIQ) and Wechsler Memory Scale (WMS-R: verbal , non verbal ,full memory) pre-operative and one year post operatively. • Changes or discrepancy of the score greater than 10 was defined as significant improvement ,changes within 10 defined as no significant changes and if lower than 10 will be considered impairment . • Also difference between Verbal and non verbal memory scores pre-operatively greater than ten was defined as verbal dominant memory impairment and vice verse or less than ten difference shows non significant laterality.
Patients & Methods Case example Pre-op Post-op Post-op gains or declines WMS-R Verbal memory 63→ 75 Non-verbal memory 82→83 Significant gain No change Pattern of memory impairment Verbal dominant VDMI No dominancy
Patients & Methods • (b) Procedures • Operative Techniques: • Two groups of patients enrolled into the study: • Group (A): Anterior temporal Iobectomy and amygdalo-hippocampectomy(14 patients). • Group (B): Selective amygdalohippocampectomy (AH) through trans-sylvian approach (10 patients). • Post operative Histopathological Studies
Patients & Methods (c) Patients' follow up • All patients will be followed up for 1-2 Years after the procedure via: • Seizure frequency every 1 month (Engel class.) • Neurological examination • Neuropsychological (WMS ,WAIS)R. • Radiologically by MRI • Electro-physiologically by inter-ictal EEG. • All the patients will be kept on anti epileptic drug regimen throughout the follow up period. Statistical methods • Data were analyzed using JMP software, version 11
Results • Preoperative status: • Age: ranged from 19 to 53yrs with mean of 34.8yrs and standard deviation of 10.9yrs
Results Demographic data and febrile seizure history in both groups
Results Seizure semiology
Results Preoperative pattern of memory impairment and side of the Temp. focus
Results The pre operative WMS-R scores • The left TLE group performed worse than right TLE group on verbal memory. But for demonstration of the pre operative non verbal memory scores were not so confirmatory
Results Seizure Outcome Engel classification
Results Seizure outcome in Engel classification according to the type of surgery • Majority of patients shows better seizure outcome after Temporal lobe epilepsy surgery. • Engel class IA (79% ATL/AH, 70% SAH), Engel II A (14% ATL/AH &10% SAH) Engle IIB (7% ATL/AH and 10% SAH) and (10%Engle IID with SAH group).
Results Seizure outcome and the duration of epilepsy • Better Engel class with patients who have shorter duration while worse control in patients with longer period (25% Engel class I, 30-36yrs),(75% Engel Class I, 8-13yrs).
Results Age of patients and seizure outcome • Young age group (19-23Y) shows 83% Engel class lA while older group (46-53Y)shows lower outcome (67% Engel class. lA)
Results Neuropsychological outcome • Intelligence Quotient (IQ) • Significant improvement in full IQ after surgery (43% ATL/AH and 30% SAH) groups with minimal impairment percent (7% ATL/AH) but the majority of patients shows no significant difference in pre-post operative Full IQ scores (50% ATL/AH and 70% SAH).