Download
1 / 150
1.5k likes | 1.74k Vues
Cardiovascular II Part 2. PVC Premature Ventricular Contraction. PVC Premature Ventricular Contraction. Premature ventricular contracture With a PVC, diastolic volume is insufficient for ejection of blood into arterial system. Therefore, no or weak pulse palpated.

E N D
PVCPremature Ventricular Contraction • Premature ventricular contracture • With a PVC, diastolic volume is insufficient for ejection of blood into arterial system. • Therefore, no or weak pulse palpated. • Few/day = OK, More/minute, the worse (>6). • Common post MI, SNS activity, K+, hypoxia.
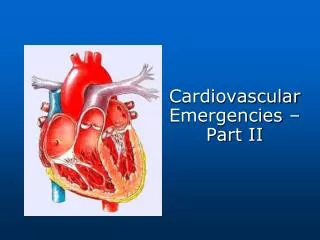
V-FibVentricular Fibrillation • Ventricle quivers but does NOT contract! • NO cardiac output and no pulses • Cardiac Arrest!! • Grossly disorganized pattern
V-TachVentricular Tachycardia • A bunch of PVC in a row • Rhythm originates below Bundle of His, in ventricular muscle. • It is too fast, so ventricular filling is ineffective and CO is ineffective • Wide, tall QRS complexes • Stops spontaneously or continues • Dangerous rhythm, diastolic filling time CO • Can cause Cardiac Arrest
Class I Antidysrhythmic Myocardium & His-Purkinje System SA Node & AV Node Lehne 5th ed Figure 47-2
Class 1B: LidocaineEffects on the Heart and the ECG • Blocks Na+ channels slow conduction thru atria, ventricles, HIS-Purkinje • Reduces automaticity -Slows the heart rate down • Accelerates repolarization (shortens action potential) • No anticholinergic effect • No change in ECG • See a restoration of sinus normal
LidocainePrecautions and Adverse Effects • Metabolized by Liver • Therapeutic range 1.5 – 5.0 microgm/ml • Pretty narrow • Adverse CNS Effects • Drowsiness, confusion, paresthesia • Toxicity • Convulsions and respiratory arrest
LidocaineAdministration • IV Push • 50-100mg (1mg/kg) • Comes in a preloaded syringe • Infusion • 1-4mg/min • Diluted in D5W • Special Considerations • Use for as short a time as possible • Reduce dosage in pts with liver disorders
Class III Antidysrhythmic • Potassium Channel Blockers:Amiodarone • Approved for V-tach and V-fib. • Delay repolarization of the ventricles Prolongs action potential and refractory period Increases PR and QT intervals - as the QT interval lengthens, the person may develop additional dysrhythmias • Initial catecholamine release brief exacerbation of dysrhythmias • - Catecholamines speed up the heart and lead to stronger heart beats • block catecholamine release vasodilation / hypotension
Class III Antidysrhythmic Myocardium & His-Purkinje System SA Node & AV Node Lehne 5th ed Figure 47-2
Non-Pharmacologic Treatment of Dysrhythmias • Cardioversion • Synchronized, coordinated shocking of the heart • Atrial fib • V-tach • Defibrillation • A shock that is delivered as soon as the buttons are pushed • V-fib
Automated External Defibrillator • Cardiac Arrest, AED “interrogates” rhythm. • Waits to see what the rhythm is and then delivers the shock as needed (timed for V-tach and not timed for V-fib.) • Tells user what to do, eg. “Shock Now” • Delivers shock for V-tach or V-fib.
Implantable Cardioverter/Defibrillator • Like a pacemaker • Monitors and analyzes rhythm • Delivers shock to terminate V-tach, V-fib
Radiofrequency Catheter Ablation • Cardiac cath and electrophysiologic (EP) test • Identify cardiac tissue site which causes dysrhythmia while in the cath lab • Map the myocardium • RF energy delivered to destroy the tissue so that that focus/area does not fire anymore • Remember, you can’t pace meatloaf • Dead myocardium or heart tissue will not respond to pacing
Antidysrhythmic DrugsSummary • Class I • Depress phase 0 in depolarization • Block sodium channels • Class II (Beta-blockers) • Depress phase 4 in depolarization • Block beta 1 & 2 adrenergic receptors HR Contractility
Antidysrhythmic Drugs: Summary • Class III (Potassium Channel Blockers) • Prolong phase 3 (repolarization) • Class IV (Calcium Channel Blockers) • Depresses phase 4 depolarization • Prolongs phases 1 & 2 repolarization
Management of Cardiac DysrhythmiasREMEMBER:Many drugs used to treat dysrhythmias also may worsen them or cause new ones!
Coronary Heart Disease andAcute Myocardial Infarction(MI or AMI)
Coronary Circulation • Two main coronary arteries arise from coronary sinus (above aortic valve) • The orifices are above the aorta • The heart perfuses during diastole because it is when the coronary arteries are open • Primary factor responsible for perfusion of coronary arteries is BP in aorta • s aortic pressure -> s coronary blood flow
Coronary Arteries • Right coronary artery • Nourishes right side, SA node, AV node – may lead to heart block • Left coronary artery • A block in the left coronary artery leads to death because it sends blood to the left side of the heart and then to the body • Left anterior descending • Left circumflex
Ischemic Heart Diseasea.k.a Coronary Heart Disease a.k.a Coronary Artery DiseaseAnginaMyocardial Infarction
Coronary Heart Disease • Heart disease caused by impaired coronary blood flow (atherosclerosis) • Cause angina, dysrhythmias, conduction defects, heart failure, sudden death, myocardial infarction (“heart attack”) • If blood flow is temporarily inadequate (due to increased oxygen demand), ischemia produces pain (angina). • Myocardial Infarction is myocardial cell/tissue death due to oxygen starvation
Assessment of Coronary Blood Flow • ECG • Exercise Stress Testing • Pharmacologic Stress Testing • May give catecholamines, such as epinephrine, norepinephrine • Nuclear Imaging • Cardiac Catheterization /Coronary angiography
Collateral Circulation • With gradual occlusion of large coronary vessels, the smaller collateral vessels in size and provide alternative channels for blood flow • Allow perfusion to the myocardium that is below and is distal to the blood flow • One of the reasons CHD does not produce symptoms until it is far advanced is that the collateral channels develop at the same time the atherosclerotic changes are occurring.
Collateral Circulation Diagram 50