Download
1 / 69
750 likes | 1.69k Vues
Carcinoma of Tongue (Oropharyngeal). Dr. Ahmed Khan Sangrasi , Assistant Professor, Dept. of Surgery, LUMHS, Jamshoro.

E N D
Carcinoma of Tongue (Oropharyngeal) Dr. Ahmed Khan Sangrasi, Assistant Professor, Dept. of Surgery, LUMHS, Jamshoro
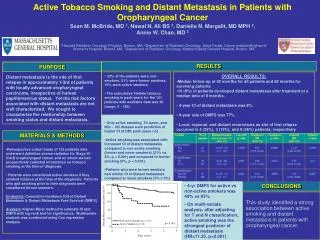
In oncology squamous cell cancers of the head and neck are often considered together because they share many similarities - in incidence, cancer type, predisposing factors, pathological features, treatment and prognosis • Up to 30% of patients with one primary head and neck tumour will have a second primary malignancy
Tobacco when kept in mouth leaches out carcinogens, which act on oral mucosa causing neoplastic changes. Habit of smoking is also equally dangerous
Tobacco contains potent carcinogens including Nitrosamines (nicotine), polycyclic aromatic hydrocarbons, Nitrosodiethanolamine, Nitrosoproline, and polonium. Tobacco smoke contains carbon monoxide, Thiocyanate, hydrogen cyanide, nicotine and metabolites of these constituents.
Tobacco in Pakistan most commonly consumed in the form of gutka, quid pan or smoking in the form of bidi of cigarette.
Gutka is a flavored tobacco mixture with betel nut lime, and harmful additives like magnesium carbonate. It is extremely addictive and is apparently targeted at youngsters. • Quid is the mixture of tobacco and lime and extensively consumed.
Precancerous lesions • There are three most common precancerous lesions seen in the mouth and they are 1.Oral leucoplakia • It is characterized by white patch on the buccal mucosa or any place in the mouth and is adjacent to the place where the tobacco quid is kept. The less likely place is floor of the mouth and tongue although 93% of leucoplakia at this sites turn malignant.
2. Erythroplakia • This is characterized by red velvety patch which is not associated with any trauma or inflammation. It may present with or without leucoplakia. This lesion is easily missed out but is considered to have great malignancy potential.
3.Oral sub mucous fibrosis. • This condition is characterized by limited opening of mouth and burning sensation on eating of spicy food. This is a progressive lesion in which the opening of the mouth becomes progressively limited, and later on even normal eating becomes difficult.
This patient of SMF has so much of limitation in opening of mouth that it is difficult to put even 2 fingers in the mouth
Professor Newell Johnson an expert oral surgeon said, ”we know this condition, oral sub mucous fibrosis has highest rate of transferring to malignancy of any of the so called pre-malignant lesions in the mouth. It is a very serious condition.”
The next stage after the precancerous lesion is the Cancerous lesions.
The most common form of cancer is Squamous cell carcinoma. • It normally starts from any of the precancerous lesion in the mouth.
Common sites of oral cancer • The most common sites of the oral cancer is the tongue and the floor of the mouth. The other common sites are buccal vestibule, buccal mucosa, gingiva and rarely hard and soft palate. Cancer of bucco-pharyngeal mucosa is common in smokers.
Cancer of Gingiva and Buccal mucosa • The lesion is usually painless in early stages and only when it becomes ulcerated and secondarily infected or invades adjacent nerve, pain is the noticeable feature. The tumor is usually at the level of the occlusal plane or below it. They may be proliferative warty exophytic growth with little fixation or deeply ulcerative invasive lesion. The proliferative lesion though it looks dangerous is easily treatable and long-term prognosis is good as the metastasis to the local lymph nodes is relatively late. Whereas the ulcerative lesion is not so easily noticeable in the early stages but is more dangerous because of their invasive nature and the metastasis to the local lymph nodes is very early
Cancer of buccal mucosa after tobacco habit going extra-orally
CANCER STARTING FROM BUCCAL VESTIBULE FOLLOWING HABIT OF PAN WITH TOBACCO
Cancer of Buccal mucosa invading extra-oral tissues following tobacco quid habit
Cancer of labial mucosa invading extra-oral tissues following tobacco quid habit
Carcinoma of the lip • Carcinoma of the lip usually starts at the vermilion border of the lower lip. 95% of lip cancer affects the lower lip. It is in the form of a nodule, which ulcerates and forms a small scab, which fail to heal completely. It is often misdiagnosed as a cold sore. Eventually the margins of the lesions become proliferative and an extensive exophytic lesion with central ulceration develops.
Cancer of palate • It is usually an ulcerative lesion and may spread extensively before involving underlying bone.
Alveolar carcinoma • Alveolar carcinoma is common in mandible that maxilla. The lesion is warty nodular and proliferative, although it may rarely present as erosive lesion. Unfortunately it mimics apical or periodontal disease and their diagnosis is often delayed. Often the neoplastic nature is recognized when socket fails to heal following dental extraction for a supposedly periodontal abscess.
Relapse caseHe was operated for cancer of lower jaw in oct ‘00
This cancer is extremely malignant and even if there is slight delay it spreads to lymph nodes of the neck. Once it spreads the prognosis becomes poor and death is inevitable and is because of erosion of major blood vessels and erosion of the base of the skull, Cachexia and secondary infection of the respiratory tract.
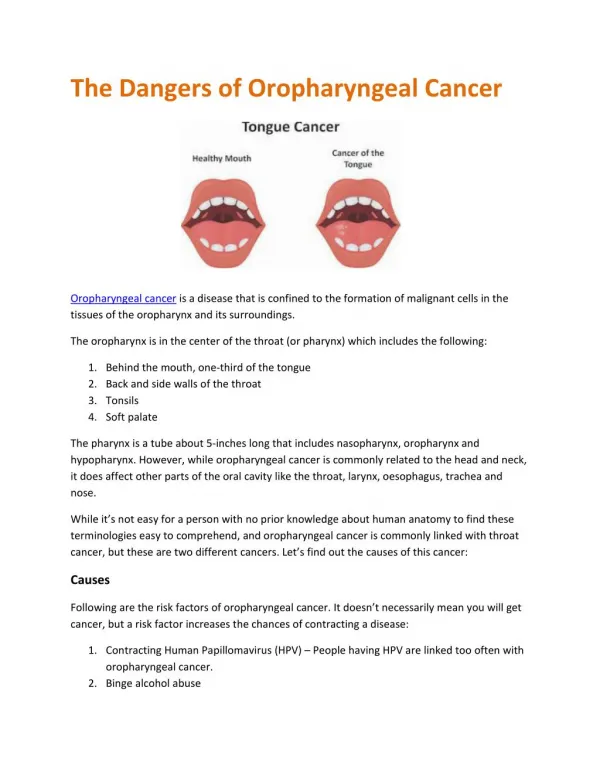
Carcinoma of the Tongue • It may start as a small ulcer, usually on the lateral border of the anterior two third of the tongue. • It may have varied presentation like a small papillary exophytic lesion, a flat nodule, ulceration within a pre existing fissure or may occur in the absence of frank ulceration in an atrophic tongue. • Once ulceration has occurred, the lesion becomes painful, making speech and swallowing difficult. • Tongue cancer rapidly extends to involve the floor of the mouth and lower alveolus, which makes treatment difficult.
Statistics on Tongue Cancer • It is relatively common, with 3% of all malignancies arising within the oral cavity • common than all forms of oral cavity cancer except those of the lip and occurs with increasing age • uncommon before the age of 40 and the highest incidence of the disease is in the 6th and 7th decades with sex incidence being a 3:1 male predominance • The disease occurs with highest incidence in Indian populations.
Progression of Tongue Cancer • tumour spreads by local extension and through the destruction of adjacent tissue • Lymphatic invasion with spread to the cervical lymph nodes is common at diagnosis • Haematogenous spread to distant sites such as the liver, bones and lungs may also have occurred at the time of diagnosis
How is Tongue Cancer Diagnosed? • General investigations may show anaemia or abnormal liver function tests if the disease is very advanced • In the early stages of tongue cancer general investigations tend to be normal. • when clinical diagnosis of oropharyngeal carcinoma is suspected a comprehensive protocol of investigations should be instituted
Investigations • Blood tests :Evaluate the patient's general health and suitability for surgery, if considered • Imaging studies : • Dental X-rays:periapical dental films provide fine details and are the most useful for detecting minimal invasion of the mandible, an orthopantomograme of the jaws is helpful to assess the bony invasion. • Chest X-ray: this may be the only useful X-ray in the evaluation for distant metastases because the incidence of distant metastases at presentation is low. • Ultrasound: Done to assess metastases of the liver.