Dr K Outhoff
Community Acquired Bacterial Infections: Principles of antibiotic therapy for common outpatient conditions. Dr K Outhoff. The scope. Goals of Antibacterial therapy Tonsillitis / pharyngitis Acute otitis media and sinusitis Community acquired pneumonia in adults Urinary tract infections

Dr K Outhoff
E N D
Presentation Transcript
Community Acquired Bacterial Infections:Principles of antibiotic therapy forcommon outpatient conditions Dr K Outhoff
The scope • Goals of Antibacterial therapy • Tonsillitis / pharyngitis • Acute otitis media and sinusitis • Community acquired pneumonia in adults • Urinary tract infections • Summary
Antimicrobial activity against a specific pathogen is reliant on: • The agent penetrating to an appropriate binding site • Attaching itself to that site in adequate concentrations • Remaining there for a sufficiently long period to inhibit bacteria from carrying out its normal life functions
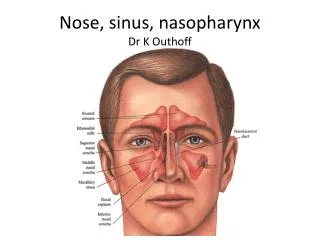
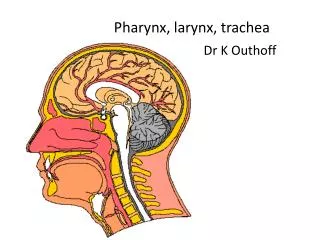
Upper and LowerRespiratory Tract Infections Tonsillitis / pharyngitis Bacterial sinusitis/ otitis media Community acquired pneumonia
Updated guideline for the management of URTIs in South Africa: 2008: SA FamPract 2009;51(2):105-114 Acute tonsillitis / pharyngitis Viral 80% Bacterial 20% Streptococcus pyogenes (GABHS) Tonsillitis Acute glomerulonephritis Rheumatic Fever • EBV • Cytomegalovirus • Adenoviruses • Measles Rx aimed at preventing above complications • Pen VK given 30 minutes before food, twice daily X 10/7 • Amoxicillin (rash if EBV present), no food restrictions, once or twice daily X 10/7 • Clindamycin if allergy • (Macrolide if allergy) Short course (3-5 days) possible with co-amoxiclav, azithro, clarithro, cefpodoxime, cefuroxime
Points in favour of empiric antimicrobial treatment • Acute onset • Temperature > 38⁰C • Tender anterior cervical nodes • Tonsillarerythema / exudates • Age 3-15 years • Previous Rheumatic -fever or -heart disease
Indications for referral Local complications: • Peritonsillar sepsis (quinsy, cellulitis, trismus) • Recurrent infections (> 4 / year) • Non-response to initial therapy Systemic complications: • Acute rheumatic fever • Severe systemic illness
Acute bacterial sinusitis / otitis media • Aetiology: • S. pneumoniae • H. Influenzae • Moraxella catarrhalis (consider if no rapid clinical response)
Antibiotic options for ABS • Beta lactams: • Amoxicillin • Amoxicillin-clavulanate • Cefuroxime* • Cefpodoxime* • Macrolides: • Erythromycin • Azithromycin • Clarithromycin • Respiratory fluoroquinolones: • Moxifloxacin • Gemifloxacin • Levofloxacin SP Oliver. Antimicrobial agents for common outpatient conditions. Mims Disease Review 2009/2010Updated guidelines for the management of URTI in SA 2008 SA FamPrac 2009
Rx: acute bacterial sinusitis • Analgesia • Antibiotics: • Amoxicillin 10 days (first choice) or • Co-amoxiclav 10 days if failed therapy • Penicilin allergy: • Macrolide • Respiratory fluoroquinolone
Indications for referral • Failure to respond after 72 hours • Peri-orbital swelling • Evidence of CNS extension (meningism, focal neuro signs, altered level of consciousness) • Severe systemic illness • Chronic sinusitis: symptomatic > 30 days
CAP • Confirm diagnosis CXR, other imaging devices • Establish aetiological diagnosis when identification of specific pathogens will significantly alter standard (empirical) management decisions. (not routine for OPD): • Sputum, microscopy, blood culture, sensitivity • Urinary antigen tests for Legionella, pneumococcus in severely ill • Endotracheal aspirate in intubated patients • Antibiotic susceptibility patterns
CAP: site of care decisions • Outpatient vs Hospital • ICU (septic shock / requiring mechanical ventilation) vs general ward • Severity-of-illness scores help identify candidates for outpatient treatment: CURB-65 criteria: confusion, ureamia, respiratory rate, low blood pressure, age 65 or greater • Prognostic scores: Pneumonia severity index (PSI) CID 2007:44 (suppl 2). Mandell et al
Community acquired pneumonia:Macrolides Addition of macrolideto beta-lactam therapy: • Appears superior to respiratory fluoroquinolonemonotherapy: • Provides coverage for atypical pathogens • Macrolides may modulate the host’s inflammatory response, even when used as monotherapy Editorial commentary , CID 2008: (15 May)
Community Acquired Respiratory Tract Infections (CARTI) • Bacterial rhinosinusitis • Acute exacerbations of chronic bronchitis (COPD) • Pneumonia • Increased resistance of Strep pneumoniae (MIC > 2 mcg/ml = high level resistance) to: • Penicillins • Macrolides (previous use of long acting macrolides) • Fluoroquinolones • Morbidity and mortality greater with PNRSP than PSSP (18.5% vs 12.2%) • Level of penicillin resistance in S. Pneumoniae at present only precludes the use of penicillin in meningitis caused by these organisms in South Africa
Risk factors for Drug Resistant S. Pneumoniae(DRSP) • Chronic comorbidity: heart, lung, liver, renal disease • DM • Alcoholism • Malignancies • Asplenia • Immunosuppressant drugs • Use of antimicrobials within last 3 months (use dif. class)
Severe CAP:combination therapy required • Ps. Aeruginosa: Piperacillin – tazobactin + fluoroquinolone • MRSA emerging as CAP pathogen: Add Vancomycin or Linezolid • Alter empiric to pathogen-directed therapy once culture results known • Switch from iv to oral once haemodynamically stable • Discharge as soon as clinically stable. • Ertapenem acceptable alternative • Telithromycin not yet adequately assessed for CAP.
Overview • Types of UTIs • Diagnosis • Pathogens • Goals of treatment • Antimicrobials • Resistant patterns
UTI • Presence of micro-organisms in the urinary tract that cannot be accounted for by contamination (> 10² /ml) • Range: asymptomatic bacteriuria to pyelonephritis with bacteraemia or sepsis • Lower Tract Infections: frequency, dysuria, suprapubic pain, haematuria • Cystitis • Urethritis • Prostatitis • Epididymitis • Upper tract Infection: flank pain, systemic illness (vomiting, fever, etc) • Pyelonephritis
Types of UTI UNCOMPLICATED COMPLICATED Predisposing lesion of the urinary tract Congenital abnormality Renal stone Indwelling catheter Prostatic hypertrophy Obstruction Neurological deficit Upper and lower urinary tract Males and females • No structural or functional abnormalities of urinary tract that interfere with normal flow of urine / voiding mechanisms • Females of childbearing age who are otherwise healthy • Lower urinary tract only
Bacteria enter the urinary tract.Factors determining development of infection: • Size of inoculum • Virulence of micro-organism • Natural host defence mechanisms
Aetiology:bowel flora of the host UNCOMPLICATED UTI COMPLICATED UTI E-coli (50%) Enterococci (esp nosocomial) Pseudomonas Klebsiella Proteus Staphylococci More resistance Sometimes multiple organisms • E-Coli (85%) • Staph. Saprophyticus (5-15%) • Klebsiella (<1%) • Proteus (<1%) • Enterococcus (<1%) • Pseudomonas (<1%) Staph Aureus from bacteraemia, causing metastatic abscesses in kidney Candida common in critically ill, chronic catheterisation
Notes on the flora:E-Coli • Increasing resistance to antimicrobials • ? 30% resistant to amoxicillin, ampicillin and cephalosporins • Oral beta lactams eliminated rapidly; • unable to reach high renal tissue concentrations compared to others • Less successful at eradicating uropathogens from vaginal and GIT reservoirs • Increasing resistance to sulphonamides • Current or recent antibiotic exposure most significant risk factor associated with E-Coli resistance
Notes on the flora:Enterococci • Extensive use of third generation cephalosporins which are not active against enterococci • Vancomycin resistant enterococci (VRE) • E. faecalis + S. faecium • Widespread • Patients after long term hospitalisation • Patients with underlying malignancies
Treatment of UTI Desired Outcome: • Treat or prevent systemic consequences of infection • Eradicate invading organism • Prevent recurrence of infection ‘The ability to eradicate bacteria from the urine is related directly to the sensitivity of the micro-organism and the achievable concentration of the antimicrobial agent in the urine.’
Rx of Acute Uncomplicated UTI Cost effective approach to management • Urinalysis • Initiation of empiric therapy • No culture Short course antibiotics • Increased compliance • Good efficacy • Fewer side effects • Lower cost • Less potential for development of resistance
UTI antimicrobial options Community acquired Severe or Hospital acquired Aminoglycosides Piperacillin-tazobactam Imipenem-cilastin • Quinolones • Fosfomycin • Nitrofurantoin • Co-amoxiclav • Cephalosporins • Co-trimoxazole
Rx UTI: cystitis Uncomplicated cystitis in non- pregnant women Asymptomatic bacteriuria Fluoroquinolone (cipro, levo, norfloxacin) Ciprofloxacin250mg stat or Ciprofloxacin 250mg bd for 3 days • Fluoroquinolone (cipro-, levo-, norfloxacin) • Ciprofloxacin 250mg stat Avoid in pregnancy
Rx UTI: Complicated cystitis • Fluoroquinolone: Ciprofloxacin for 3 days • Co-amoxiclav for 7 days • Nitrofurantoin for 7 days • 2nd generation cephalosporin: cephalexin, cefuroxime for 7 days
Rx UTI: pyelonephritis Uncomplicated pyelonephritis Culture Outpatient 14 day course of oral • Fluoroquinolone - ciprofloxacin
Rx UTI: pyelonephritis Complicated pyelonephritis (Culture, admit. ) 14 days: start intravenous, switch to oral when afebrile • Fluoroquinolone • Extended spectrum penicillin + aminoglycoside Hospital acquired, catheter, nursing home: Pseudomonas • Antipseudomonas penicillin + aminoglycoside