Sore Throat
E N D
Presentation Transcript
1. Sore Throat Miss N Su
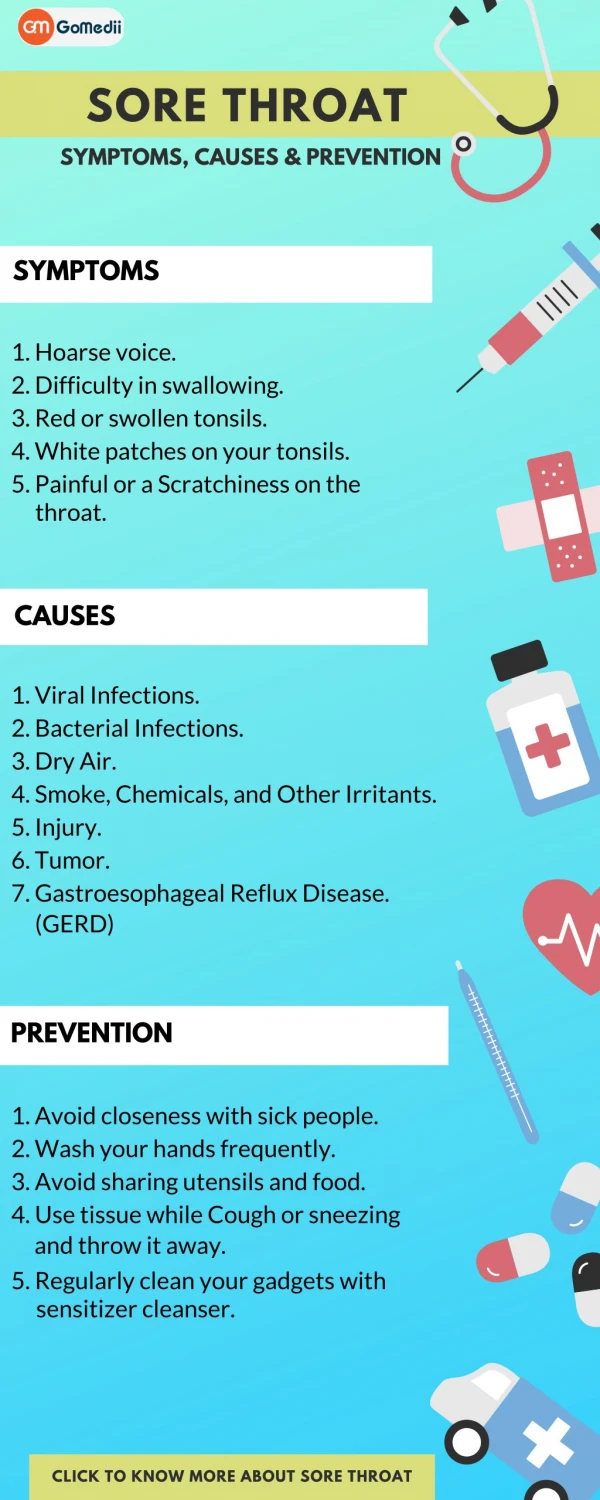
2. To cover the broad topic of �sore throat�, focusing on conditions of the oropharynx Aims
3. Accidental biting, other trauma and burns all cause mouth ulcers.
These should heal within 7-14 days
Any patient with a single mouth ulcer persisting for greater than 2-3 weeks should have it further investigated.
Mouth ulcers
4. Common, reoccurring episodes of ulcers, usually from childhood or adolescence
Aggravating factors: stress, trauma, cessation of tobacco smoking
10-20% have an underlying haematological pathology
Recurrent Aphthous stomatitis
5. Recurrent aphthous stomatitis plus genital ulceration and eye disease
Genetic background
Males 30-40yrs most commonly affected
Treated with colchine, steroids and immunosuppressants
Bechet�s syndrome
6. What viruses cause oral ulceration?
7. Herpes simplex virus
Herpes zoster (look for immunocompromise in young patients
EBV
Coxsaccie virus (herpangia or hand foot and mouth) A
8. During what stage of syphilis would you find oral ulceration? Bacterial infections
9. Primary syphilis � primary hard or huntarian chancre
Secondary � mucous patches and snail track ulcers
Tertiary � localised granulation - gumma All 3 stages may present with oral lesions
10. TB Rare but can present with oral lesions- ulceration of dorsum of tongue described as an irregular ulcer with a granulating base. Looks similar to and SCC
11. Overlaps with the common cold, mild form with low grade fever is assoc with rhinovirus, coronavirus and RSV.
More severe form is assoc with fever, sore throat, malaise, pharyngitis and cervical lymphadenopathy � caused by adenovirus, influenza virus, enterovirus, EBV, herpes simplex and HIV Viral Pharyngitis
12. 6 yr old boy
48hr history of sore throat, pyrexia and malaise
O/E T 38.5 , bilateral tender cervical lymphadenopathy and enlarged erythematous tonsils. Patient 1
13. Bacterial
Group A beta-haemolytic streptococcus
Groups C and G beta-haemolytic streptococcus
Viral
Rhinovirus
Corona virus
Respiratory syncytal virus
Parainfluenza
EBV
Fungal
Candida albicans
You make a diagnosis of tonsillitis � what are the possible pathogens?
14. Supportive treatment with fluids
Calpol
?antibiotics
Need to avoid aspirin due to risk of Reye's syndrome
Avoid ampicillin How would you manage this patient?
15. Rheumatic fever 0.3% of untreated Pxs
Post strep glomerulonephritis
Abscess formation
Septacaemia
Acute OM / mastoiditis
Lemierre syndrome
Complications of GABHS
16. Rheumatic fever occurs in 0.5-3% of ineffectively treated patients with GABHS.
Occurs approx 20 days after the sore throat.
Diagnosed on the presence of 2 major criteria, or 1 major criteria and 2 minor criteria
Rheumatic fever
17. Antibiotics should not be used to routinely prevent from developing RF or glomerulonephritis
Antibiotics do improve symptom control, but only marginally compare to simple analgesia- increased benefit in symptoms occurred 16 hours earlier in patients given antibiotics The role of antibiotics in sore throat
18. Age range 14-25yrs
Tonsillitis with thick exudate and palatal petechiae .
Up to 50% develop splenomegally
5% have a rash, this will increase to 90% if given ampicillin or amoxicillin.
Treatment is largely supportive, can lead to airway compromise requiring tonsillectomy or even tracheostomy EBV infection- infectious Mononucleosis
19. Name 3 different causes of exudate on the tonsils
How can you tell these conditions apart?
20. Glandular fever
Vincent�s angina
Diphtheria
If you scrape the exudate off in diphtheria the underlying mucosa bleeds, the underlying mucosa in Vincent�s is erythematous but doesn�t bleed. Answer
21. Present in the unimmunised population
Causes a greyish exudate extending
from the tonsils to soft palate
Spreads via respiratory droplets and
infected objects or food
Mortality rate remains 5-10%
Toxins can cause cardiac and neural toxicity
Treatment involves antitoxin and penicillin or erythromycin Diphtheria
22. Primary HIV infection can cause an acute retroviral syndrome:
Fever
Non-exudative pharyngitis
Arthralgia
Malaise and lethargy
Macculopapular rash in 40-80%
HIV
23. Idiosyncratic drug reaction, may present with fever and sore throat.
Diagnosed on FBC
Drugs implicated:
Antiepileptics
Antithyroid drugs
Antibioitcs � penicillin, chloramohenicol, co-trimoxale
Cytotoxic drugs
Gold
NSAIDs
Some anti-depressants and anti-psychotics Agranulocytosis
24. Acute Leukaemia All forms may present with nonspecific sloughing ulcers on the gums, oral cavity and pharynx and possible cervical lymphadenopathy
Diagnosis is based on blood film and bone marrow examination
25. What is the differential diagnosis?
Unilateral tonsil enlargement
26. Malignancy - asymmetry in normal tonsil � in the absence of cervical lymphadenopathy has a 7% risk of malignancy
Chance or malignancy if mucosa abnormality or lymphadenopathy is very high
Rare tumours
Extramedullary plasmacytomas
Hodgkin�s disease
Leukaemia and metastatic deposits
Infection- candida and actinomycosis
Quinsy /parapharyngeal space mass
Unilateral tonsil enlargement
27. What is the differential diagnosis? Tonsil ulceration
28. Neoplastic � SCC, salivary gland tumours, lymphoma, melanoma, myeloma
Infection � acute strep inf, quinsy, diphtheria, EBV and CMV mononucleosis and Vincent's angina
Chronic- syphilis, TB and AIDs
Blood disorder- agranulocytosis, leukaemia
Miscellaneous: aphthous ulceration, Bechet�s syndrome, colloidal bismuth intoxication Tonsil ulceration
29. Indications for tonsillectomy for recurrent tonsillitis
sore throats are due to tonsillitis;
the episodes of sore throat are disabling and prevent normal functioning.
Seven or more episodes in the preceding year
Or five or more episodes of sore throat per year for 2 years
3 or more episodes for the last 3 years
Tonsillectomy
30. Asymmetrical adult
For obstructive sleep apnoea (OSA) in children in conjunction with adenoidectomy is a well-recognized .
In adults with gross tonsil hypertrophy and OSA, or as part of uvulopalatopharyngoplasty (UPPP) or laser-assisted uvulopalatoplasty.
Severe haemorrhagic tonsillitis.
Severe infectious mononucleosis with upper airway obstruction.
Large symptomatic tonsoliths (tonsillar concretions).
As long-term management of IgA nephropathy. The long-term prognosis is no longer regarded as benign but with pulsed steroid therapy and tonsillectomy significant increases in clinical remission rates can be obtained (25 percent with tonsillectomy, 13 percent without) also with significant increases in renal survival.49,?50,?51,?52
Other indications for tonsillectomy
32. History of long standing sore throat and discomfort of variable severity.
Possible aetiology:
Heavy smoking
Chronic rhinosinusitis with increased post nasal drip
Laryngeal pharyngeal reflux
Poor dental hygiene
Chlamydia pneumonia
Chronic pharyngitis