Download
1 / 83
830 likes | 1.02k Vues
SPUC – Neuropathology Cases 10-31-2011. B.K. Kleinschmidt-DeMasters, MD. CASE 1. The patient is a 58-year old woman with a right parieto-occipital mass. Referring pathologist's diagnosis was oligodendroglioma. . Monotonous cell population Multifocal calcifications, many concentric

E N D
SPUC – Neuropathology Cases 10-31-2011 B.K. Kleinschmidt-DeMasters, MD
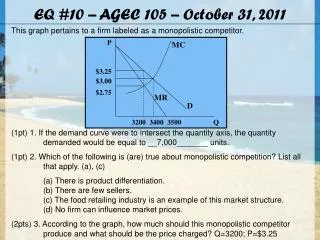
CASE 1 • The patient is a 58-year old woman with a right parieto-occipital mass. Referring pathologist's diagnosis was oligodendroglioma.
Monotonous cell population • Multifocal calcifications, many concentric • Cytologically relatively bland nuclei • No necrosis, pseudopalisading necrosis, microvascular proliferation • No microcysts
Minimal GFAP+ fibrillar cytoplasm surrounding most small cells GFAP
Tumor IDH-1 negative (left) • Positive control shown at low at medium power shown at (right) for comparison IDH 1
Nuclear p53 <5% • MIB-1 15% (medium and high power) p53 MIB 1
CASE 1 The patient is a 58-year old woman with a right parieto-occipital mass. Referring pathologist's diagnosis was oligodendroglioma. Special Studies? Differential Diagnosis
CASE 2 • The patient is a 35-year-old male with a left frontal lobe, 7.3 x 5.8 cm, enhancing mass. Tumor was extremely heterogenous, necrotic and/or cystic, and produced prominent left-to-right midline shift.
Arcuate vasculature Necrosis Monotonous population
Areas of tumor with microvascular proliferation Monotonous cells with rounded, highly eosinophilic cytoplasm
Vascular thromboses Arcuate vasculature grouping tumor in almost endocrine-like fashion
Significant nuclear atypia Nuclei not completely uniform; some angular
Mitotic activity Prominent nucleoli, almost metastatic carcinoma-like
Distinctly different regions with same nuclei but prominent, ball-like eosinophilic cytoplasm
Nuclei maintain similar features to the other areas of tumor
Minimal GFAP immunoreactivity in one area • Where present often shows ball-like cytoplasm with rounded profiles, few stellate processes GFAP
Other areas are strongly GFAP immunoreactive but cytoplasmic profiles are rounded, lack stellate blunted cell processes GFAP
Nuclear p53 <5% MIB-1 is 20% IDH-1 is positive in case 2 MIB 1 p53 IDH 1
Features seen elsewhere in same tumor: Nuclear palisades (‘en filade’)
Features seen elsewhere in same tumor: Very focal calcification; chunky
CASE 2 The patient is a 35-year-old male with a left frontal lobe, 7.3 x 5.8 cm, enhancing mass. Tumor was extremely heterogenous, necrotic and/or cystic, and produced prominent left-to-right midline shift. Additional special Studies Differential Diagnosis
CASE 3 • The patient is a 61-year-old female who has a left basal ganglion mass, which, at the time of frozen section, was interpreted as metastatic carcinoma. The patient has a significant past medical history of endometrial carcinoma.
Permanent sections made the referring pathologist nervous about their original diagnosis
Permanent sections made the referring pathologist nervous about their original diagnosis
Nuclear monotony Apparently uni-modal cell population Prominent nucleoli
Scant cytoplasm Mitotic activity Little or no necrosis, microvascular proliferation
Permanent section of the frozen section that the referring hospital had to work with
FS1 is clearly from an aggressive tumor; note the mitotic figures
CASE 3 The patient is a 61-year-old female who has a left basal ganglion mass, which, at the time of frozen section, was interpreted as metastatic carcinoma. The patient has a significant past medical history of endometrial carcinoma. Special Studies Differential Diagnosis
CASE 4 • The patient is a 30-year-old female with a posterior fossa / fourth ventricular, 1.6 x 2.3 cm enhancing lesion that was partially cystic and solid, and involved the cerebellar vermis and extended into the right medial aspect of the right cerebellar hemisphere.
Infiltrating monotonous tumor cells Some perivascular Seemingly uni-modal cell population B
Brisk mitotic activity visible in areas of better cytological preservation B
Areas with more angular nuclei Note occasional nucleoli B
AFS 1 this is what the referring pathologist had to deal with
CASE 4 The patient is a 30-year-old female with a posterior fossa / fourth ventricular, 1.6 x 2.3 cm enhancing lesion that was partially cystic and solid, and involved the cerebellar vermis and extended into the right medial aspect of the right cerebellar hemisphere. Special Studies Differential Diagnosis
CASE 5 • The patient is a 51-year-old female with a 4.2 x 4.5 cystic mass in the cerebellum.
B Cerebellar granular cell neuronal layer should not be mistaken for medulloblastoma especially on frozen section or touch preparation
B Sausage shaped structures surround this tumor type frequently
Some areas of tumor are very bland and do not even look like a neoplasm B
Other areas of tumor have glassy cytoplasm and low N/C ratio B