Exercise Treadmill Testing
Exercise Treadmill Testing. Prognostication in Coronary Artery Disease Dr. Peter Krampl 11 October 2001. Introduction. 300,000 ER visits per year acute non traumatic chest pain Only apx. 25% have clear positive, Unstable coronary disease Angiography Image studies

Exercise Treadmill Testing
E N D
Presentation Transcript
Exercise Treadmill Testing Prognostication in Coronary Artery Disease Dr. Peter Krampl 11 October 2001
Introduction • 300,000 ER visits per year acute non traumatic chest pain • Only apx. 25% have clear positive, • Unstable coronary disease • Angiography • Image studies • Acute myocardial infarction • or negative diagnosis of coronary syndromes
Introduction • Current ED Modalities • Reviewed in EM Clinics February 2001 • History / Physical • Mair. Chest. 1995. • 110 patients; non traumatic chest pain • Using NPV as most used indicator for admission • PPV 53% NPV 75% for acute cardiac ischemia
Introduction • Current ED Modalities • ECG • Rovan, American Journal Cardiology. 1989. • Multicentre Chest Pain Trial • Sensitivity 61% Specificity 90% for ischemia • Current ST, Q, LBBB criteria • Variable Specific • Addition of T wave abnormality • Sensitivity increases to 95% • Specificity may decreases to 23% • Current computer algorithms tend to higher sensitivity
Introduction • Current ED Modalities • Cardiac Markers • Hedges et al. Acad EM. (CK-MB) • 1042 patients; CK-MB at presentation and serial investigated • Sensitivity 19-31% Specificity 95-96% • Hamm et al. NEJM. 1997 (TnT) • 776 patients • Prospective study looking at prognosis of TnT and TnI and 30 day cardiac event rate • Negative values of T and I gave annual event rates of 1.1 and 0.3% respectively • Sensitivity 31% Specificity 98%
Introduction • Are We Satisfied With Those Numbers? • How Do We Further Risk Stratify Coronary Patients? • Treadmill Testing • Observation Units / Time • Radionuclear Imaging +/- Exercise • Echocardiography +/- Exercise • Angiography
Introduction • In ED, old chart or patient notes: • I was on treadmill for 8 minutes. • A negative treadmill. • I did not have pain on the treadmill. • What do those mean? • Can we use those simple guides to further stratify these patients?
Outline • Introduction • Treadmill Testing • Review of Current Literature • Introduction • Indications • Procedures • Results • Notable Studies • Exercise Modalities • Conclusions • Questions
Treadmill Testing: Introduction • Froelicher. Hdbk of Exercise Testing. 1996 • Goals • Diagnosis CAD • Prognosis CAD • Evaluation of Medical Therapy • Evaluation of Exercise Capacity
Treadmill Testing: Indications • When to use…. • AHA / CPSA guidelines advise to use only up to intermediate pre test probability cases • Kuntz et al. Ann Int Med. 1999. • Exercise stress test or rest echo most cost effective (mild-mod) • Life expectancy • Cost • Incremental Cost Effectiveness over other modalities • For high risk, immediate coronary angio most cost beneficial. • Other stress modalities supplement to Exercise Treadmill
Treadmill Testing: Indications • Braunwald et al. High / Intermediate / Low Risk / Pretest Probability Guidelines published by AHA 1995. Reviewed by Primary Care Clinics. 2001 • Example: Low Risk • Chest pain by history classified as “probable not or definitely not angina • normal ECG • New onset angina 2 months • No change in previous 2 months • T wave flattening or inversion <1 mm in leads with dominant R waves • One risk factor other than diabetes
Treadmill Testing: Indications • Majority of tests done on referral basis • Advent of chest pain units in United States… • Studies by • Zalenski. Ann EM. 1997. Low and Intermediate Risk. • Safety at 4-12 hours • Mikhail. Ann EM. 1997. Intermediate risk. • Safety at 12 to 24 hours • Lewis. Am J Card. 1994. Low risk. • Safety at 1-2 hours • Kirk. Ann EM. 1998. Low risk. • Safety at 1-2 hours • CP Observation Units have adopted 6 hours as Industry standard for exercise port work up and stabilization
Treadmill Testing: Indications • Indications • Froelicher / Annals of EM • Clear (Class 1) • Evaluation of male patients with atypical symptoms • Functional capacity testing • Evaluation of exercise related dizziness, syncope, palpitations • Evaluation of Recurrent exercise induced Arrhythmias
Treadmill Testing: Indications • Indications • Probable Benefit (Class 2) • Evaluation of Women with atypical symptoms • Evaluation of Variant Angina • All those in Class one with baseline ECG changes other than LBBB • Evaluation of patients on digitalis or RBBB
Treadmill Testing: Indications • Indications • Not Indicated (Class 3) • Assymptomatic young men / women with no risk factors and high suspicion non cardiac chest discomfort • Evaluation of patients with LBBB • Evaluation of Patients with Pre-excitation Syndromes
Treadmill Testing: Indications • Contraindications • AHA Guidelines • Absolute • AMI within 3-5 days • Unstable angina not stabilized by medical therapy • Aortic dissection • Endo, Myo, or pericarditis • PE • Lower Extremity Thrombosis • Uncontrolled symptomatic cardiac arrhythmias • Severe aortic stenosis • Symptomatic severe and terminal heart failure
Treadmill Testing: Indications • Contraindications • Relative • High degree AV block • Moderate stenotic valvular disease • DBP >200 or DBP > 110 • Bradyarrythmias • Known left main coronary stenosis • Mental / physical incapacity
Treadmill Testing: Indications • Complications • Brady / Tachyarrythmias • AMI / Sudden Death • CHF / Shock • MSK Trauma / Fatigue / Malaise
Treadmill Testing: Procedures • Important Concepts • VO2 max : maximum oxygen uptake • Amt of O2 transported for cellular metabolism • Useful to express in multiples of METS • CO X (arteriovenous oxygen difference) • METS used to standardize protocols • MO2 : myocardial O2 uptake • wall tension, thickness, contractility and HR • Estimated by double product (HR X BP) • Angina usually occurs at the same double product
Treadmill Testing: Procedures • Physiology • Exercise creates increase CO • Four to six fold increase from rest at peak • CO increase by increase HR and PB and decreased vagal tone • HR affected by • Age, sex, motivation, habitus, blood volume, health • SBP increases with exercise • DBP stays same or slightly decreases • Hypotension ominous sign • Outflow obstruction, ventricular dysfunction or ischemia
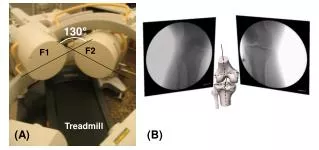
Treadmill Testing: Procedures • Equipment • Treadmill or cycle ergometer • Cycle has major pitfall of rapid fatigue of quadriceps in older patients • Most studies use treadmill • Handrails, Rest Area • Assistant, Supervisor • Resuscitation Equipment
Treadmill Testing: Procedures • Preparation • Fast 3 hours prior / dress appropriately… footwear • Medications reviewed by physician prior • History and physical prior regarding change in disease • CHF; valvular disease; onset of unstable angina; bronchospasm • Consent • Baseline supine and upright ECG
Treadmill Testing: Procedures • Protocols • Most diagnostic and prognostic studies based on Bruce protocol • Seven phases • Change in grade and speed every 3 minutes • Correlation with METS • Large incremental stages • Not correlated for height / weight / stride • Ideal protocol lasts 6-12 minutes and adjusts for patients ability • Others include Naughton, McHenry, USAF, Blake
Treadmill Testing:Procedures • Borg Scale • Borg. Sports and Exercise. 1982. • Correlation of scale to actual fatigue • 6-20 grade scale for exertion • 10 grade scale for exertion now adopted • 0 – nothing • 9 – very strong • 10 – very, very strong • Continues to be a clinical assessment of fatigue by technician (skilled) and supervisor • Mainly used as repetitive assessment tool in rehab
Treadmill Testing: Procedures • Measurements • ST depression / elevation (60-80 ms; J point changes) • ST slope (downsloping worse than horizontal) • Duration of changes into recovery • Exercise induced arrhythmias • Peak HR / BP • Total Duration • Exertional hypotension • Angina • Other exercise induced symptoms
Treadmill Testing: Procedures • Termination • Absolute • Drop of SPB > 10 • Anginal Pain (other than non-limiting / known pain) • CNS symptoms • Signs of poor perfusion • Serious Arrhythmias (runs of VT > 3; multiform) • Technical Difficulties in monitoring • Subject Request
Treadmill Testing: Procedures • Termination • Relative • Maintenance of SBP well into protocol • Excessive ST / QRS changes • Fatigue, SOB, Wheeze, Cramps, Claudication • SVT • Development of BBB • Observation Important !! • Case 77 y.o. male; level one indications; no contraindications; stable angina • Maintenance of SBP into Phase 2
Treadmill Testing: Results • Diagnostic • Exercise Treadmill (ST response only) Sens 66% Spec 84% Froelicher et al. Exercise. 1993. Sens 70% Spec 75% Gianrossi. Meta-analysis. Circulation. 1989. Using Bayes rules of pretest probability, these numbers may only be applied to intermediate cases at best. • Original Duke University Investigators showed repeated studies of poor specificity and positive predictive value
Treadmill Testing: Results • Diagnostic • Lehmann and Froelicher. Veteran’s Study Group. QUEXTA. Ann Int Med. 1998. • 814 patients • 400 selected for decreased work-up bias • Only 40% Stress test ‘positive’ ST changes correlated to > minimal luminal CAD • Overall sensitivity 45% specificity 85%
Treadmill Testing: Results • Prognostic • Giagnoni. NEJM. 1983 • Prospective following of 135 men with ST changes vs. 379 controls • Angina, MI, sudden death endpoints • 5.55 percent risk increase • Suggested that ECG positive ST changes should be independent coronary risk factor
Treadmill Testing: Results • Prognostic • Mark et al. Duke University. Ann Int Med 1987; • Validation Mark et al. NEJM. 1991. • Developed score based on 613 patients (1983-85) • Validated on further 1420 patients • Simple score to prognosticate patients • Associated score > 5 with annual mortality of • 0.25 % outpatients • 0.6 % inpatients
Treadmill Testing: Results • Prognostic • Duke Score • Time in minutes • ST depression in mm • Type of pain 0 - none 1 – typical anginal pain limited by time / fatigue / other 2 – limiting anginal pain
Treadmill Testing: Results Duke Score = Time(m) – 4X Angina – 5X depression(mm) Score: 5 & above low risk 4 to –9 intermediate risk -10 & below high risk
Treadmill Testing: Results • Kowk et al. JAMA. 1999. • Revisited Duke Score • 2405 patients • 939 had ST segment changes on stress test • Found 97 % seven year survival based on score Duke > 5 • These studies have solidified the prognostic benefits of the treadmill test
Treadmill Testing: Results • Duke score • Low Risk • Less than 1% per year acute coronary syndrome • Optimize Medical Rx; reassess in one year • Intermediate Risk • 1 to 5 % per year • Optimize Medical Rx; nuclear studies non-urgent • High Risk • Greater than 5 % per year • Urgent referral for further risk stratification
Treadmill Testing: Results • Other prognostic indices: • Morrow & Froelicher. Ann IM. 1993. • Veteran’s Score • Exercise duration • ST depression • Rate of change of systolic BP during exercise • History of CHF, digoxin use • Low risk groups stratified with 2% annual mortality
Treadmill Testing: Results • Exercise Capacity • AHA Guidelines • Carliner et al. Am J Card. 1985 • Reasonable to Use exercise testing for • Surgical patients recovering from • Congenital repair • Valvular replacement • Cardiac transplant • CHF • DM • CRF • Chronic Lung Disease • No exercise induced symptoms
Treadmill Testing: Results • Exercise Capacity and Prognostication • Lauer and Fletcher. Circulation. 1996. • 1575 men; mean age 43 • Failure to achieve 85 % of age predicted maximum heart rate • associated with increase in death of 1.84 • Extrapolation techniques used
Treadmill Testing: Results • AHA Guidelines • Evaluation of Medical Therapy • Look for improvement of exercise capacity to previous before angina or ST depression • Evaluation of Valvular Disease • Strict guideline for evaluation of AS • Evaluation of Dysrrythmias • PVC, Sick sinus Syndrome • Pre-operative • Anesthetists 2nd largest user of stress test for evaluation of patient for non cardiac surgery
Notable Studies • Exercise Hypotension • Dubach et al. Circulation. 1989 • Looking at SBP drop with exercise • Looked at 0, 10, 20 drop of SBP • Drop of 20 associated with increased PPV of at least 50% Left Main or Triple Vessel Disease
Notable Studies • Variables • Prakash et al. Am Heart J. 2001 • 3974 men • Kaplan-Meier regression • Four variables predict mortality within 5 year • Rate of change of rate-pressure product • Age > 65 • Maximum MET <5 • LVH on ECG
Notable Studies • METS • Ramamurthy et al. Chest. 1999. • Found that sensitivity increases if MET >7 • Also found that METS achieved may be a stronger variable than rate-pressure product • High heart rate at low MET (<5) level carries adverse prognosis
Notable Studies • Risk Factors • Am J Cardiol. MRFIT. 1985. • Multiple Risk Factor Intervention Trial • 12,866 participants • Those with ST changes on Stress Treadmill benefit to greater degree with risk factor modification than controls.
Notable Studies • Women • Large number of false positives • Mitral valve prolapse; • Higher incidence atypical chest pain • Hormonal, esp. estrogen mimickery of digoxin • Ventilation Responses and Metabolic Alkalosis • Curzen. Heart. 1998. • 205 women • Compared with coronary angiography • 42 false positives & 31 false negatives (36 % of total) • Increase false positives correlated with • Increasing age to 52 • Increasing coronary risks to 3
Notable Studies • Early Stress Testing • Polanczyk. Am J Card. 1998. • 276 low risk patients • Stress test within 48 hours • Similar prognostication numbers • 0.5 % event rate • Additional variables over 6 months • 15% less ED visits • 30% fewer admission
Exercise Modalities • Stress Echocardiography • Evaluate rest / stress changes in wall motion. • Dobutamine given to stimulate beta-1 • Advantages: Readily available; little equipment; transportable • Disadvantages: poor images in up to 10%; user dependant; hard in presence of previous abnormalities
Exercise Modalities • Thallium 201 • Older agent; Replaces potassium in cells • Advantages • Able to calculate lung heart ratios • Disadvantages • Immediate imaging • Poor in obese patients and large breasted women • Maddahi. Am J Coll Card. 1989 • Increases sensitivity from 60-70% of treadmill test to 90% overall with addition of perfusion studies but 70% with single vessel disease
Exercise Modalities • Technetium-99m sestamibi • Deposited into mitochondria • Advantages • Longer half life • Better images • Improved estimates of ejection fraction • Disadvantage • Poor extraction from blood at high blood flow • Hachamovitch et al. Circulation. 1996. • 834 patients; treadmill, Tc-99m and catheterization • 78% of the listed 0.6% mortality from Duke Low Treadmill prognostication caught as severe perfusion scans.
Exercise Modalities • Two schools of thought: • EM Clinics Feb 2001 • “as useful as exercise testing is, it has the limitations of suboptimal sensitivity and specificity…. Imaging is a necessity, not an optional component of stress testing” vs. “exercise testing alone is a useful first step.” • Froelicher. Primary Care. 2001. • Quotes George Bernard Shaw “the doctor does the test he is paid the most for” to stress our need for continued evaluation of present modalities