
Desquamative Gingivitis and Its Clinical Manifestations
E N D
Presentation Transcript
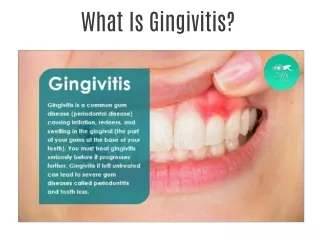
Desquamative gingivitis • clinical term • red, painful, glazed and friable gingiva manifestation of some mucocutaneous conditions such as lichen planus or the vesiculobullous disorders
gingival epithelium that spontaneously sloughs or can be removed with minor manipulation
The differential diagnosis includes • Specific mucocutaneous dermatoses such as • benign mucous membranepemphigoid (BMMP) • erosive (bullous) lichen planus • systemic lupus erythematosus • pemphigus vulgaris • Paraneoplastic pemphigus • erythema multiforme • Epidermolysis bullosa acquisita • Chronic ulcerative stomatitis • linear immunoglobulin (Ig) A disease, • and a nonspecific group of hormonal or idiopathic origin
desquamative gingivitis with vesiculobullous erosive lesions of other oral-mucosal tissues andconjunctival eye lesions benign mucous membrane (cicatricial) pemphigoid.
Clinical Features • Cicatricial pemphigoid usually affects older adults, with an average age of 50 to 60 years at the onset of disease. • Females are affected more frequently than males by a 2:1 ratio. • Oral lesions are seen in most patients, but other sites, such as conjunctival, nasal, esophageal, laryngeal, and vaginal mucosa, as well as the skin may be involved. The oral lesions of pemphigoid begin as either vesicles or bullae that may occasionally be identified clinically In contrast, patients with pemphigus rarely display such blisters.
Mucous Membrane Pemphigoid:The full thickness of epithelium has separated from the corium, which is edematous and infiltrated by inflammatorycells • A routine biopsy specimen displays a subbasal epithelial–connective tissue split
Mucous Membrane Pemphigoid: • Immunofluorescent studies show linear basement membrane deposits of IgG and complement (C3)
Erosive lichen planus Desquamative gingivitis in a patient with other oral erosions +peripheral zones of white reticulated striae
Clinical feature • more significant for the patient because the lesions are usually symptomatic. • Clinically, there are atrophic, erythematous areas with central ulceration of varying degrees. The periphery of the atrophic regions is usually bordered by fine, white radiating striae
A biopsy specimen exhibits a subbasal split with a subepithelial, bandlike lymphocytic infiltrate.
saw-toothed rete ridges, and a bandlike infiltrate of lymphocytes immediately subjacent to the epithelium. A
In immunofluorescenttesting of the submitted tissues: • Globular deposits of C3 and fibrinogen are seen in the basement membrane
Desquamative gingivitis in a patient with extensive large bullous and erosive lesions throughout the oral mucosa and skin pemphigus vulgaris
Clinical Features The initial manifestations of pemphigus vulgaris often involve the oral mucosa, typically in adults. The average age at diagnosis is 50 years, although rare cases may be seen in childhood Patients usually complain of oral soreness, and examination shows superficial, ragged erosions and ulcerations distributed haphazardly on the oral mucosa Such lesions may affect virtually any oral mucosal location, although the palate, labial mucosa, buccal mucosa, ventral tongue, and gingivae are often involved. Patients rarely report vesicle or bulla formation intraorally, and such lesions can seldom be identifie by the examining clinician, probably because of early rupture of the thin, friable roof of the blisters. Over 50% of the patients have oral mucosal lesions before the onset of cutaneous lesions, sometimes by as much as 1 year or more. Eventually, however, nearly all patients have intraoral involvement. The skin lesions appear as flaccid vesicles and bullae that rupture quickly, usually within hours to a few days, leaving an erythematous, denuded surface. Infrequently ocular involvement may be seen, usually appearing as bilateral conjunctivitis.
PARANEOPLASTIC PEMPHIGUS (NEOPLASIAINDUCEDPEMPHIGUS) vesiculobullous disorder that affects patients who have a neoplasm, usually lymphoma or chronic lymphocytic leukemia.
A suprabasal epithelial split is seen on a routine biopsy examination Pemphigud Vulgaris:an ulcer with an intact basal cell area.
immunofluorescence exhibits: intercellular IgG deposits Pemphigus Vulgaris: immunofluorescence staining with anti-IgG shows deposit along the intercellular borders of the epithelium and coating acantholytic cells.
Extensive hemorrhagic-crusted lesions of the lips; erythematous circular iris or target lesions on the skin;a wide variety of intraoral, erythematous, and vesiculoerosive lesions, in conjunction with desquamative gingivitis • Erythema multiforme
A biopsy specimen demonstrates: a nonspecific suprabasal and subbasal epithelial split Immunofluorescent studies are generally negative
Desquamative gingivitis in a patient with pruritic vesiculobullous skin lesions, ocular lesions, and/or perineal involvement Linear IgA disease
A biopsy specimen showsa subbasal epithelial–connective tissue split. Immunofluorescent studies demonstrate linear deposits ofIgA and fibrin in the basement membrane.
Epidermolysis bullosa acquisita • autoantibodies directed against type VII collagen • Oral lesions are present in nearly 50% of the cases, although such lesions are uncommon in the absence of cutaneous lesions • To distinguish epidermolysis bullosa acquisita from other immunobullous diseases with subepithelial clefting, a special technique is performed: A sample of the patient's perilesional skin is incubated in a concentrated salt solution; this causes the epithelium to separate from the connective tissue, forming an artificially induced bulla. • Immunohistochemical evaluation shows : deposition of IgGautoantibodies on the floor of the bulla. This finding is in contrast to that of most forms of cicatricial pemphigoid, in which the autoantibodies are usually localized to the roof of the induced blister
Chronic ulcerative stomatitis • It may appear as desquamative gingivitis or as ulcerations of the tongue or buccal mucosa The histopathologic features of chronic ulcerative stomatitis are similar to those of lichen planus, the epithelium is generally more atrophic and the inflammatory infiltrate contains plasma cells and lymphocytes.
Its characteristic immunopathologic pattern, however, consists of autoantibodies directed against the nuclei of stratified squamous epithelial cells. Both direct and indirect immunofluorescence studies are positive for these antibodies, which recently have been shown to react with a p53-like nuclear protein. Unlike the lesions of erosive lichen planus, the lesions associated with chronic ulcerative stomatitis are less responsive to topical or systemic corticosteroid therapy. Management with hydroxychloroquine has been recommended.
Chronic cutaneous lupus erythematosus • The oral manifestations of CCLE essentially appear clinically identical to the lesions of erosive lichen planus • Unlike the oral lesions of lichen planus, however, the oral lesions of CCLE rarely occur in the absence of skin lesions. An ulcerated or atrophic, erythematous central zone, surrounded by white, fine, radiating striae, characterizes the oral lesion of CCLE Sometimes the erythematous, atrophic central region of a lesion may show a fine stippling of white dots. As with erosive lichen planus, the ulcerative and atrophic oral lesions of CCLE may be painful, especially when exposed to acidic or salty foods.
A patient with desquamative gingivitis without any other lesions or systemic symptomology • Nonspecific, chronic desquamative gingivitis of hormonal or idiopathic origin
A biopsy shows a subbasal epithelial–connective tissue splitimmunofluorescence is completely negative