Download
1 / 69
690 likes | 826 Vues
Intelligent Use of Anticoagulants. Murray L. Shames, M.D. Assistant Professor of Surgery and Radiology Division of Vascular and Endovascular Surgery. Outline. Available anticoagulants Surgical prophylaxis DVT and pulmonary embolus Atrial fibrillation

E N D
Intelligent Use of Anticoagulants Murray L. Shames, M.D. Assistant Professor of Surgery and Radiology Division of Vascular and Endovascular Surgery
Outline • Available anticoagulants • Surgical prophylaxis • DVT and pulmonary embolus • Atrial fibrillation • Perioperative management of patients on chronic anticoagulation • Arterial thromboembolism • Cerebral • Visceral • Extremity • Anticoagulation in pregnancy
The Coagulation Cascade Intrinsic system XII XIIa XI IX Xia IXa + VIIa + Ca++ Extrinsic system Injury Tissue thromboplastin + VII X Xa + Va + Ca++ Prothrombin Thrombin Fibrinogen Fibrin
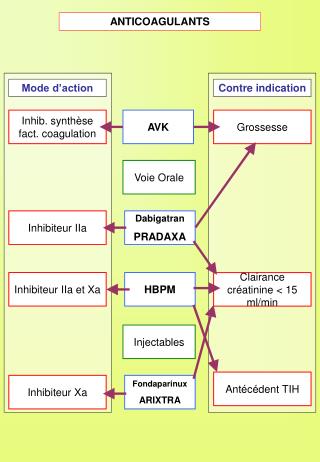
Available anticoagulants • Unfractionated heparin • Low Molecular Weight Heparins • Oral Anti-coagulants • Alternative agents
Unfractionated Heparin-Mechanism of Action • Binds anti-thrombin III 1:1 • Inactivates thrombin and F Xa • Secondary effect on F V • Effects not first order kinetics • Effective after subcutaneous and intravenous administration • Short half life (90 min) • Reversed with protamine (1mg per 100 U circulating heparin)
Unfractionated Heparin-Limitations • Significant protein binding • Response is unpredictable (close monitoring required) • <25% of patients in therapeutic range 12 hours after starting Rx • Inaccessibility of clot-bound thrombin
Unfractionated Heparin-Dosing • Loading 80-100 U/ kg IV • Then IV infusion at 18 U/kg/hr • Normogram available for most hospitals • Therapeutic range 1.5-2.5 X control PTT
Unfractionated Heparin- Complications • Major bleeding complications 0-7% • HIT 1-5% • Osteoporosis • Alopecia • Hypoadrenalism • Anaphylaxis
Heparin – Induced Thrombocytopenia • Incidence 1-5% • Can occur with all methods of administration • No known risk factors • Increased incidence with Bovine preparations • Dx- plt count < 100-150 000/uL
Heparin – Induced Thrombocytopenia I • HIT I • Heparin induced platelet aggregation • Platelet sequestration and consumption • Mild • Thrombocytopenia in first few days of therapy • Plt count usually > 100 000/uL • Asymptomatic • Resolves spontaneously without d/c heparin
Heparin – Induced Thrombocytopenia II • HIT II (HITT) • Immunologically mediated • Ab to Heparin-PF 4 complex • More severe but less common • 5-7 days after initiating Tx • PLT << 100 000/uL • Bleeding complications unusual • Diffuse thrombotic events • Separate and distinct from initial event requiring heparin Rx
Heparin – Induced Thrombocytopenia II • Thrombotic events arterial and venous • Associated skin necrosis • Global amnesia • Prosthetic valve thrombosis • 29% mortality and 21% amputation rate
Heparin – Induced Thrombocytopenia –Treatment • Withdrawal of ALL heparin and heparin products • Plasmapheresis - anecdotal success • Further treatment should await confirmation of Dx • Start anti-platelet therapy • ? LMWH • Thrombin inhibitors • Ancrod • Conversion to Warfarin
Available Anticoagulants • Unfractionated heparin • Low Molecular Weight Heparins • Oral Anti-coagulants • Alternative agents
Characteristics of UFH and LMWH Chains 5,400 10,000 5,000 15,000 20,000 Molecular weight (daltons) Anti-Xa Anti-IIa and anti-Xa Resistant to PF4 Sensitivity to PF4 Little non-specific binding Non-specific binding Inhibition of thrombin generation Less inhibition thrombin generation Hirsh J, Levine MN. Blood. 1992; 79: 1-17.
Low Molecular Weight Heparins • Effect through AT III • Inhibits Factor Xa • More predictable anticoagulant response • Longer half-life • Better bioavailability at low doses • Renal clearance • Lower incidence of HIT • No need to monitor PTT in most cases
FDA-Approved Indications (May 2001) for Available LMWHs
Advantages of LMWH Over UFH • Less platelet activation • Less vascular permeability • Smaller size • Increased release of TFPI from vascular endothelium • Less plasma protein binding • Less interaction with PF4 • Less osteoclast activation • Less binding to VWF • Stimulates megakaryopoiesis • Less thrombin, growth factor production • May limit tumor movement into intravascular space • More potent anti-angiogenesis activity • More potent anticoagulant and anti-cancer activity • Predictable PK, safety, once daily dosing • Lower incidence of HIT • Less osteoporosis with long term use • Less bleeding • May attenuate chemotherapy - induced thrombocytopenia
Low Molecular Weight Heparins- Dosing • 1mg/kg q12H • Can monitor anti-factor Xa levels
Available Anticoagulants • Unfractionated heparin • Low Molecular Weight Heparins • Oral Anti-coagulants • Alternative agents
Oral Anticoagulation- Mechanism of Action • Inhibition of Vitamin K-dependant coagulation factors II, VII, IX, X • Inhibition of Vitamin K- dependant carboxylation of Protein C and S
Oral Anticoagulation-Limitations • May create initial hypercoaguable state • 3-5 days for anticoagulant effect • 3-5 days to reverse effects • Reversed rapidly by FFP • Can reduce time of reversal with supplemental Vit K (10mg IV or 3-5mg PO)
Oral Anticoagulation-Complications • Hemorrhage • Skin necrosis • Protein C deficiency • Malignancy • Teratogenic
Oral Anticoagulation- Dosing • Loading 5mg PO QD • Adjust daily dose to reach goal INR
Available Anticoagulants • Unfractionated heparin • Low Molecular Weight Heparins • Oral Anti-coagulants • Alternative agents
Alternative Anticoagulants • Danaproid • Thrombin Inhibitors • Hirudin • Lepirudin • Argatroban • Ancrod
Alternative Anticoagulants-Danaproid • Heparinoid • Mixture heparin-like glycosaminoglycans and chondroitins • Anti-factor Xa and anti-factor IIa activity • Can be used in patients with HIT • Approved for DVT prophylaxis • Longer duration than UF heparin • Measure by anti-factor Xa levels • Weight based dosing
Alternative Anticoagulants-Thrombin Inhibitors • Hirudin • Protein isolated from salivary gland of leech • Irreversible binding to thrombin • High incidence of bleeding complications • Monitor by PTT and ACT • Substitute for heparin in patients with HIT • Efective DVT prophylaxis
Alternative Anticoagulants-Thrombin Inhibitors • Lepirudin • Recombinant Hirudidn derivative • Reduced mortality and morbidity in HIT patients • Renally excreted • Dosing - 0.4mg/kg IV loading and 0.15mg/kg maintenance • Monitor PTT • Therapeutic range: 1.5 – 2.5 X normal
Alternative Anticoagulants-Thrombin Inhibitors • Argatroban • Competitive thrombin inhibitor • Univalent thrombin inhibitor (less specificity and affinity) • Short plasma life- no adj. for RF • 2ug/kg/min IV • Monitor by PTT or ACT (2-3.5 X baseline)
Alternative Anticoagulants-Ancrod • Venom of Malaysian Pit Viper • Defibrinating agent • Converts fibrinogen to soluble aggregate removed by plasmin and RES • Increases FDP – augments anticagulant effect • Indirect micro-fibrinolytic by increasing TPA release • Monitor fibrin levels
Venous Thromboembolism Virchow’s Triad • Stasis • Intimal injury • Activation of coagulation (hypercoaguable state)
Venous Thrombosis-Epidemiology • Venous thromboembolism is the 3rd most common vascular disease in the United States • Mortality and morbidity associated with VTE is enormous • Average cost per admission in the US: • PE = $12,595 • DVT = $9,337 • Additional long-term costs of morbidity > 75% of initial therapy costs
Venous Thrombosis-Rationale for Prophylaxis • Clinically “silent” disease • High prevalence in hospitalized patients • Dire consequences of missed DVT • First manifestation may be fatal PE • Most deaths within 30 min of acute event • Long term morbidity from post-phlebitic syndrome • Wide variations in practice of physicians • Only 1/3 of at risk patients receive adequate prophylaxis • 58% of fatal PE patients not prophylaxed in spite of risk factors
Obesity Varicose Veins Cardiac dysfunction Indwelling vascular catheter IBD Nephrotic syndrome Pregnancy or estrogen use Advanced age Prolonged immobility Stroke or Paralysis Previous VTE Cancer and its treatment Major Surgery esp. abdomen, pelvis, and lower extremities Trauma esp. fractures of pelvis, hip, or leg Venous Thrombosis- Risk Factors
Surgical Prophylaxis-Low Risk Patient • Risk Factors • Age under 40 years • Minor surgery • No other risk factors • Event rate • Calf DVT 2.0% • Proximal DVT 0.4% • Clinical PE 0.2% • Fatal PE 0.002% • Recommended Regimens • No specific measures • Aggressive mobilization
Risk Factors Major surgery in patients with additional risk factors Non-major surgery in patients 40-60 with no additional risk factors Major surgery in patients < 40 with no additional risk factors Event Rates Calf DVT 10-20% Proximal DVT 2-4% Clinical PE 1-2% Fatal PE 0.1-0.4% Surgical Prophylaxis-Moderate Risk Patient • Recommended Regimens • LMWH • Low dose UFH • Elastic stockings • Intermittent Pneumatic Compression
Risk Factors Non-major surgery in patients > 60 or additional risk factors Major surgery in patient < 40 or additional risk factors Event Rate Calf DVT 20-40% Proximal DVT 4-8% Clinical PE 2-4% Fatal PE 0.4-1.0% Surgical Prophylaxis-High Risk Patient • Recommended Regimen • LMWH • Low dose UFH q8h • IPC
Risk Factors Major surgery in patients > 40 plus prior VTE, cancer, hypercoaguable state Hip or knee arthroplasty Major trauma Spinal cord injury Event Rate Calf DVT 40-80% Proximal DVT 10-20% Clinical PE 4-10% Fatal PE 0.2-5.0% Surgical Prophylaxis-Highest Risk Patient • Recommended Regimen • LMWH • Oral Anticoagulants • IPC/ES + LMWH/LDUFH • Adjustable dose UFH
Deep Venous Thrombosis-Treatment • Start LMWH (SC enoxaparin 1mg/kg q12h or 1.5mg/kg q24) and warfarin • Stop LMWH after 4-5 days when INR > 2.0 for 2 consecutive days • Continue warfarin for at least 90 days at INR 2.0-3.0
LMWH vs. UFH In Acute Treatment of VTE Venous Thromboembolism Pulmonary Embolism Major Bleeding Minor Bleeding Total Mortality Thrombocytopenia 0.0 0.25 0.5 0.75 1 1.5 1.25 0.75 2 In Favor of LMWH In Favor of UFH Pooled Relative Risk Dolovich L, et al. Arch Intern Med. 2000:160:181-187.
LMWH: Fewer Deaths Meta-Analysis: N=3,566 LMWHUFH P Mortality 5.1% 6.7% 0.02 Overall 30% mortality reduction from: Recurrent Thromboembolism, Bleeding, and Cancer Gould, et al. Ann Intern Med. 1999; 130: 800-9.
Outpatient Treatment of DVTEnoxaparin q12h vs. Heparin Study Design Enoxaparin sodium 1mg/kg q12h SC Clinical endpoints Documented acute, proximal DVT without PE Adjusted-dose heparin infusion Clinical endpoints Warfarin 90 days post randomization Warfarin therapy initiated on 2nd day
Outpatient Treatment of DVTEnoxaparin q12h vs. Heparin Results: Recurrences of Thromboembolism Heparin n=254 (%) Enoxaparin sodium n=247 (%) Embolic Event Total VTE* DVT only Proximal DVT PE 13 (5.3)† 11 (4.5) 10 (4.0) 2 (0.8) 17 (6.7) 14 (5.5) 12 (4.7) 3‡ (1.2) *VTE = venous thromboembolic event (deep vein thrombosis [DVT] and/or pulmonary embolism [PE]). † 95% CI = -5.6 to 2.7. ‡ Two died during the study.
Outpatient Treatment of DVTEnoxaparin q12h vs. Heparin Results: Episodes of Major Bleeding aPTT (sec) INR* Study Day Treatment Group & Event Enoxaparin sodium (n=5)† Soft-tissue hematoma of hip 6 2.7 27 Abdominal-wall hematoma 7 2.7 55 Abdominal-wall hematoma 7 3.2 40 Subdural hematoma 5 3.4 40 Hematemesis‡ 6 2.4 40 Heparin (n=3)† Hematuria 2 1.3 64 Gastrointestinal bleeding 3 3.0 88 Hematemesis 1 2.7 64 * International Normalized Ratio. †P = 0.50. ‡ Patient had cancer and associated thrombocytopenia due to chemotherapy and radiation.
Atrial Fibrillation • Most common arrythmia in adults • Responsible for 15% CVA • Better survival with combined rate control and anticoagulation • IV heparin/ LMWH + coumadin • Administer anticoagulation before and 3 - 4 weeks after cardioversion
Atrial Fibrillation Risk Factors For Stroke* None None 1 or more Therapy ASA or none ASA or Warfarin Warfarin Age < 65 >65-75 Any *Mitral stenosis, HTN, previous TIA or stroke, CHF, LV dysfunction, or age > 75
Perioperative Management Of Patients on Chronic Anticoagulation Patients at low risk • VTE adequatelt treated for > 3 months, no predisposing factors • Nonvalvular A. Fib without embolic events • Most bioprosthetic and mechanical heart valves without thromboembolism
Perioperative Management Of Patients on Chronic Anticoagulation Recommendations • Hold warfarin 4 days before surgery • Recheck PT day of surgery • Resume warfarin on post-op day 2
Perioperative Management Of Patients on Chronic Anticoagulation Patients at intermediate risk • Venous or arterial embolism • In 2nd to 3rd month of Tx, no predisposing factors • Recurrent VTE tx for 12 months • Valvular heart disease, A. Fib, prosthetic heart valve with distant h/o embolism