Download
1 / 29
300 likes | 602 Vues
Assessing Behavioral Disorders in the Geriatric Population. Long Term Care Dementia 50-70% Affective disorders 10-15% Schizophrenia 0-4% Mental retardation/ Developmental disabilities 1-5%. What Are the Most Common Psychiatric Disorders in the Elderly?. Outpatient Care

E N D
Long Term Care Dementia 50-70% Affective disorders 10-15% Schizophrenia 0-4% Mental retardation/Developmental disabilities 1-5% What Are the Most Common Psychiatric Disorders in the Elderly? Outpatient Care • Dementia 10% > age 65 45% > age 85 • Depression 4-5% • Substance abuse 1-5% • Psychosis 0.1-4%
50 40 30 20 10 0 Prevalence of Dementia in the US • >65 years: 10% • >85 years: 32% to 47% • Today: About 4 million have Alzheimer’s Disease (AD) • 2050: Greater then 14 million will have AD • Economic burden associated with AD approaches $100 billion annually 32 Prevalence of Dementia (%) 16 8 4 2 1 60-65 65-70 70-75 75-80 80-85 >85 Age (year)
Over age 65 5% live in nursing homes now 25% to 50% will live in nursing homes at some point in their lives Over age 85 25% live in nursing homes Prevalence of mental disorders in nursing homes is estimated to be more than 75% Nursing Facilities Demographics • Currently, there are 17,176 nursing homes in the US • There are more than 1.5 million residents • Hospitals are releasing patients sooner; nursing homes are taking a larger role in sub acute care Rovner BW, et al. Am J Psychiatry. 1986;143:1446-1449. American Health Care Association. 1998. Available at: http://www.ahca.org
Dementia:A Diagnostic Workup • Medical history • Medication history • Social history • Psychiatric history • Neurological exam • Mental status exam • Blood test • Imaging studies (eg, optional CT without contrast, MRI, PET, SPECT)
Differential Diagnosis of Dementia • Alzheimer’s disease (AD) • Dementia with Lewy bodies (DLB) • Frontotemporal dementias • Dementia with Parkinson’s disease • Vascular dementia • Other degenerative dementias
Required Laboratory Studies • Complete blood count • Serum electrolytes (including calcium) • Glucose • BUN and creatinine • Liver function tests • TSH and free thyroid index • Vitamin B12 level • Syphilis serology
Lumbar Puncture • Early onset, rapidly progressive or unusual features • Metastatic carcinoma • Suspicion of normal pressure hydrocephalus • Increased tau, decreased beta-amyloid (sensitivity/specificity unknown)
Functional QEEG SPECT PET fMRI MRS Examples of Imaging Techniques • Structural • CT • MRI
Parietal/temporal deficits Focal, asymmetric, cortical subcortical deficits Parietal deficits Frontal/global deficits What Functional Imaging Can Show • Alzheimer’s disease • Vascular dementia • Parkinson dementia • Depression
IPA Consensus Statement Behavioral signs and symptoms of dementia are • Common • Morbid • Classifiable • Treatable Finkel SI, et al. Int Psychogeriatr. 1996;8(suppl 3):497-500.
Behavioral Scales Used to AssessNeuropsychiatric Symptoms in Dementia • Behavioral Pathology in AD Scale (BEHAVE-AD) • ADAS non-cognitive subscale (ADAS-non-cog) • Behavioral Rating Scale for Dementia (BRSD) • Cohen-Mansfield Agitation Inventory (CMAI) • Columbia University Scale for Psychopathology in Alzheimer’s Disease (CUSPAD) • Brief Psychiatric Rating Scale (BPRS) • Neuropsychiatric Inventory (NPI)
Behavioral Disturbances Associated With Dementia % of Patients Range Median 0-86 19 Disturbed affect/mood Disturbed ideation 10-73 33.5 Altered perception Hallucinations 21-49 28 Misperceptions 1-49 23 Agitation Global 10-90 44 Wandering 0-50 18 Tariot PN, et al. Am J Psychiatry. 1993;150:1063-1069.
Range Median 11-51 24 Resistive/uncooperative 0-46 14.3 27-65 44 Anxiety 31.8 Withdrawn/passive behavior 21-88 Sleep 0-47 27 Diet-appetite 12.5-77 34 Behavioral Disturbances Associated With Dementia (cont.) (% of Patients) Aggression Verbal Physical 0-50 61 Vegetative behaviors Tariot PN, et al. Am J Psychiatry. 1993;150:1063-1069.
Neurobiology of Behavioral Disturbances in Dementia Ach • Cholinergic function, related to neural mechanisms of emotion • Controversial link between dementia severity and agitation • Mixed findings regarding role in mood disorders • Decreased activity associated with psychotic features • Some behavioral benefit associated with cholinergic treatment
Neurobiology of Behavioral Disturbances in Dementia (cont.) 5HT • Decreased 5HT more pronounced in behavior disturbances • Depression associated with decreased activity • Psychosis history associated with decreased activity • Agitation associated with decreased activity and agonist challenge • Serotonergic agents show mixed results
Neurobiology of Behavioral Disturbances in Dementia (cont.) NE • Increased NE responsivity may contribute to behavioral disturbances • Increased NE turnover in depression and psychosis • Decreased NE in depression? • May suggest avoiding noradrenergic agents in treatment • May support use of -blockers
Neurobiology of Behavioral Disturbances in Dementia (cont.) DA • Relative preservation in aggression • No relationship to mood disturbance • No relationship to psychosis • Agitation correlated with plasma HVA • Antipsychotics may be more effective in decreased aggression than psychotic features in AD • Significant deficit in LBD
Neurobiology of Behavioral Disturbances in Dementia (cont.) GABA • GABA deficit well established in AD • Little known about changes in behavioral disturbances • Decreased activity associated with aggression in animals • GABA modulators and benzodiazepines have moderate effect • Role of anticonvulsants
Neurobiology of Behavioral Disturbances in Dementia (cont.) Corticotropin Releasing Factor (CRF) • Decreased activity in neurodegenerative disorders • Relevant to stress response • Many pharmacotherapies modulate CRF Glutamate • Imbalance between glutamate and dopamine may lead to psychosis
What Is Agitation? • Any inappropriate verbal, vocal, or motor activity that is not an obvious expression of need or confusion Cohen-Mansfield J, Deutsch LH. Semin Clin Neuropsychiatry. 1996;1:325-339.
Agitation Physical Verbal Pacing Inappropriate robing/disrobing Trying to get to a different place Handling things inappropriately Restless Stereotypy Complaining Requests for attention Negativism Repeated questions, phrases Screaming Cohen-Mansfield, et al. 1988.
Aggression Range Median Characteristic Verbal 11% to 15% 24% Threats Accusations Name-calling Obscenities Physical 0% to 46% 14% Hitting Kicking Pushing Scratching Tearing Biting Spitting Sexual 18% in 1 report
General Approach to Behavioral Complications of Dementia • Characterize target symptoms • Standard medical evaluation to identify possible medical disorder • If medical disorder, treat and monitor target symptoms • Standard psychiatric evaluation • If psychiatric disorder, treat and monitor target symptoms
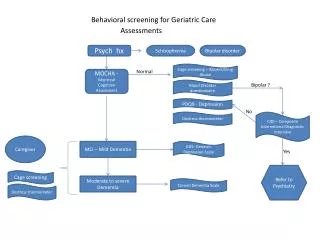
Flow Chart for Management of Agitation in Dementia Agitation No Acutely manageable? Short-term sedation with antipsychotics, benzodiazepines Yes Effective? Medical workup No • Hospitalize • Restraints? • Seclusion? Specific medical disorder • Treat specifically • Monitor agitation • Employ nonpharmacologic principles Yes Delirium Yes Discrete psychiatric disorder No Tariot, et al. Tariot and Leibovici.
Flow Chart for Management of Agitation in Dementia (cont.) Employ nonpharmacologic principles Continue treatment as appropriate Yes Develop psychobehavioral metaphor, match to relevant class, continue attempting nonpharmacologic approaches No Successful? Depressive features Anxious features Nonspecific Manic features Psychotic features Antidepressants Anticonvulsants Anticonvulsants Antidepressants Anticonvulsants Anxiolytics Empirical trials of appropriate agents Antipsychotics No Effective? • Continue as appropriate • Consider eventual empirical withdrawal Yes Tariot, et al. Tariot and Leibovici.
Nonpharmacologic Approaches • Modify environment • Optimize stimulation • Use consistent routines • Assess/adapt to aggravating factors • Behavior management principles • Education • Support of patient and caregivers
General Approach to Pharmacotherapy • Use psychotropics where appropriate • Empirical trials of symptomatic pharmacotherapy for remaining symptoms • Start low, go slow • Assess target symptoms and toxicity • Increase dose until benefit or toxicity • Hold at nontoxic efficacious dose or subtoxic dose; levels may help
General Approach to Pharmacotherapy (cont.) • If effective, continue for weeks to months, taper and re-evaluate • If ineffective, taper and re-evaluate; consider second agent • Medications do not always work