Download
1 / 27
270 likes | 445 Vues
Adult Swallowing EBP Group. Extravaganza Presentation 2009 In patients with dysphagia is there a relationship between oral hygiene and pneumonia? Does the evidence confirm our suspicions?. Who are we?. The adult swallowing EBP Group comprises of both metropolitan and rural members.

E N D
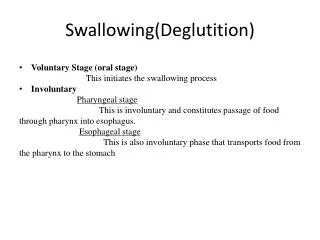
Adult Swallowing EBP Group Extravaganza Presentation 2009 In patients with dysphagia is there a relationship between oral hygiene and pneumonia? Does the evidence confirm our suspicions?
Who are we? The adult swallowing EBP Group comprises of both metropolitan and rural members. We are practicing Speech Pathologists with a particular interest in the management of adult swallowing impairments.
Forming our Clinical Question… Areas of interest… • Oral Hygiene • Tongue Strengthening exercises
Signs of poor oral hygiene • Plaque and debris • Development of infections in the mouth such as mouth ulcers • Dental caries • Loss of teeth • Pain and discomfort in the mouth • Altered taste
Signs of poor oral hygiene • Dry mouth • Fissures of the tongue • Inability to wear dentures • Periodontal disease • Halitosis (Rieger et al 2005; Roberts 2000)
What are our suspicions? • For those of you who work in the area of dysphagia please raise your hand if you include oral care as part of your swallowing recommendations. • Why do we do this? • What is it that we suspect? • We suspect that there is a relationship between oral hygiene and pneumonia in patients with dysphagia.
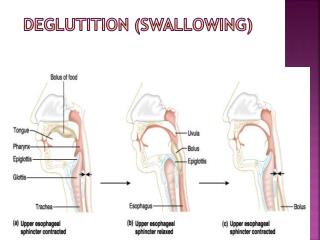
Flow chart of pneumonia development • Dysphagia & pneumonia: a complex relationship (Langmore 1998) • Colonisation (altered oropharyngeal flora): • Aspiration into lungs • Host resistance • Pneumonia
Clinical Question In patients with dysphagia is there a relationship between oral hygiene and pneumonia?
Searching for Evidence • Search terms: Oral hygiene, Pneumonia, Aspiration pneumonia, Dysphagia, Swallowing, Mouth Care, Oral Care. • Databases: Medline, Embase, CIAP, PsychINFO, CINAHL and Science direct • Other resources Google Scholar, reference lists of other articles/texts. • Area Librarians.
Critically Appraised Papers • Over 120 articles initially identified • 65 were actually accessible • 17 initially thought to be relevant • 3 articles deemed relevant during formation of CAT
Quagliarello, V., Ginter, S., Han, L., Van Ness, P., Allore. H., & Tinetti, M. (2005). Modifiable risk factors for nursing home-acquiredpneumonia. Clinical Infectious Diseases, Vol 40 pp: 1-6 • Level of Evidence: IV • Prospective study;613 nursing home residents over the age of 65 underwent surveillance for 12 months post enrolment in the study, or until an end point was reached (i.e. diagnosis of pneumonia or exclusionary event).
Results: Quagliarello et al • 16% of pneumonia cases could have been prevented if adequate oral care had occurred. • 5% of pneumonia cases could have been prevented if swallowing difficulty had not occurred. • In patients with > two risk factors at baseline,35% of pneumonia cases may have been prevented if adequate dental care occurred. 38% of pneumonia cases may have been prevented if swallowing difficulty had not occurred • 21% of pneumonia in the entire cohort could have been prevented if inadequate oral care and swallowing difficulties had not occurred.
Clinical Bottom Line: Quagliarello et al • Oral hygiene and swallowing difficulties were identified as two modifiable risk factors that could prevent development of nursing home acquired pneumonia. • Patients do not need these risk factors to occur simultaneously for pneumonia to develop. • Management of oral hygiene and swallowing difficulties may reduce the risk of pneumonia.
Langmore, S, E. Terpenning, M, S. Schork, A. Chen, Y. Murray, J. T. Lopatin, D, Loesche, W. J. (1998) Predictors of Aspiration Pneumonia: How important is Dysphagia? Dysphagia Vol 13 pp: 69-81 • Level of evidence: III.2 • Prospective outcomes study design; 160 males >60yrs, diagnoses of CVA, other neurological conditions, gastrointestinal disease, diabetes, COPD, congestive heart failure. Subjects were followed for four years for an outcome of aspiration pneumonia. • All participants underwent; clinical and fluoroscopic examination, dental exam and scintigraphy examination on an annual basis. Half of the participants also underwent FEES if indicated • Medical & functional status was also collected.
Results: Langmore et al • 81% of all subjects with aspiration pneumonia had oropharyngeal dysphagia, 58% aspirated liquid, 27% aspirated food and 50 % aspirated their own secretions. • 46% of patients with nil dentition (edentulous) also developed pneumonia. • 16% Bed bound patients developed pneumonia, • 43% patients with reduced activity levels developed pneumonia. • 41% of patients dependent upon other to feed them developed aspiration pneumonia.
Clinical Bottom Line: Langmore et al • Aspiration pneumonia can not be attributed to a single causal factor; it is the result of a variety of predictors experienced in conjunction. • Dysphagia and aspiration are necessary factors but the most significant predictors were; • dependence for feeding and oral hygiene, • number of decayed teeth, • enteral feeding, • co- morbidities, • quantity of medications, and • smoking.
Ferozali F, Johnson G & Cavagnaro A. Health Benefits and Reductions in Bacteria from Enhanced Oral Care. Special Care in Dentistry 27: 5, 2007. • Level of evidence: II • Randomised control study: 36 subjects, ages 31-79. Subjects followed for 90 days. • Participants had one or more of the following inclusion criteria, enteral feeding, hiatal hernia, emesis, GORD or swallowing difficulties. • Participants were divided into 3 groups; group1 underwent oral cleansing with suctioning, group 2 underwent teeth cleaning with sodium bicarbonate, group 3 was the control with no additional intervention received. • Oral health was evaluated 3 times during the study using a simplified Beck Oral Assessment tool. Condition of the lips, oral mucosa, gingival tissue and plaque was scored by the Dental Hygienist who was blinded to group membership.
Results:Ferozali et al • All groups demonstrated reductions in number of hospitalisation days for respiratory infections • Reducing the level of bacteria in the mouth likely reduces the risk of infection and upper respiratory tract illness. • The majority of potentially pathogenic bacteria was detected in the mouths of subjects receiving PEG feeds when compared to overall group. • Suctioning in collaboration with oral care is beneficial
Clinical bottom line: Ferozali et al • Oral care combined with intermittent suctioning may reduce respiratory infections for long term care residents with multiple risk factors including swallowing difficulties that place them at high risk of aspiration pneumonia.
Strengths in the evidence: Langmore, et al • Overview of literature • Use of gold standard tool in the confirmation of the presence of aspiration Quagliarello et al • The modifiable risk factors were comprehensively assessed. The pneumonia outcome definition was rigorous and included radiographic evidence. • Use of intra observer reliability testing of both modifiable risk factor assessment and pneumonia outcome detection. • Evaluating the fraction of cases of pneumonia that could have been prevented by modifying each risk factor Ferozali et al • Random assignment of subjects • Inclusion of microbiologists and dental hygienists.
Limitations in the evidence: Langmore et al • Nil specific documentation of whether fluids were modified • Small subject sample • Subjects are only male veterans. Quagliarello et al • Only using lack of dental examination as the definition of inadequate oral care. • The use of cough during swallow as the definition of swallowing difficulty ignores patients who silently aspirate oropharyngeal contents. • Only baseline assessment of modifiable risk factors. • No measures of external validity. • Paper focused on nursing home acquired pneumonia • Nil comparison of modifiable risk factors amongst participants who did and did not develop pneumonia. Ferozali et al • Number of patients with or without dysphagia were not identified. • short duration and small sample size of study. • Oral care still undertaken in control group.
Clinical Implications • Oral hygiene and dysphagia are risk factors that can be attributed to the development of pneumonia, if we can manage or minimise these risk factors the risk of developing pneumonia can be reduced. • “Therefore clinicians managing patients with dysphagia need to look beyond their traditional therapy approaches of changing posture, training swallowing manoeuvres and altering diet and consider more indirect approaches such as training family members, nurses and volunteers who feed patients in providing good oral care and facilitating dental treatment for patients with dental disease” (Langmore et al 1998).
CAT 2: Progress Report • We have also been busy working on a second CAT this year. • Do tongue strengthening exercises effect the impaired oropharyngeal swallow? • So far… 60 articles evaluated • 10 relevant articles found so far • CAPs to get underway early 2010 • Watch this space!!
Where to next year? • Completion of CAT 2 • Free Water Protocol? • The ageing swallow?
Contacts • Please feel free to contact us if you would like to join the group: • Christine Button cbutton@stvincents.com.au • Jessica Newman jnewman@nsccahs.health.nsw.gov.au • Anna Corry acorry@nsccahs.health.nsw.gov.au (until the end of 2009) • Please contact us if you are interested in co-leading the group • Refer to the EBP website for more details about the group.
References • Ferozali F, Johnson G & Cavagnaro A. Health Benefits and Reductions in Bacteria from Enhanced Oral Care. Special Care in Dentistry 27: 5, 2007. • Langmore, S, E. Terpenning, M, S. Schork, A. Chen, Y. Murray, J. T. Lopatin, D, Loesche, W. J. (1998) Predictors of Aspiration Pneumonia: How important is Dysphagia? Dysphagia Vol 13 pp: 69-81 • Quagliarello, V., Ginter, S., Han, L., Van Ness, P., Allore. H., & Tinetti, M. (2005). Modifiable risk factors for nursing home-acquired pneumonia. Clinical Infectious Diseases, 40, 1-6. • Rieger, J., Seikaly, H., Jha, N., Harris, J., Williams, D., Liu, R., McGraw, T. & Wolfaardt, J. (2005). Submandibular Gland Transfer for Prevention of Xerostomia After Radiation Therapy. Archives of Otolaryngology and Head and Neck Surgery, 131, 140-145. • Roberts, J. (2000). Developing an oral assessment and intervention tool for older people: 1. British Journal of Nursing, 9(17), 11241127.