EEG
EEG. For Neurology Residents 2009. Not exactly EEG, but…. …things you need to know. Epilepsy and driving. Epilepsy and pregnancy. OUTLINE. I. What is an EEG and how is it recorded ? II. How do you read an EEG ? III. The use of EEG IV. Slideshow/Quiz. PART I.


EEG
E N D
Presentation Transcript
EEG For Neurology Residents 2009
Not exactly EEG, but… …things you need to know. • Epilepsy and driving. • Epilepsy and pregnancy
OUTLINE I. What is an EEG and how is it recorded ? II. How do you read an EEG ? III. The use of EEG IV. Slideshow/Quiz
PART I WHAT IS AN EEG AND HOW IS IT RECORDED?
Recording procedure 20-30 minutes, relaxed patient Eyes opened/closed Photic stimulation, Hyperventilation +/- sleep +/- pain, noise
PART II HOW DO YOU READ AN EEG ?
Why do you need to know this? • Exams • Emergencies • To understand the reports
An organized approach • Orient yourself. • Is there normal brain activity present or is it altered ? • Is there abnormal activity present ? • What is the state ? • Is it age – appropriate ? • Are there any artifacts present ?
1. ORIENT YOURSELF Montage (bipolar or referential) F7, F8 Time scale Sensitivity (amplitude, positive/negative) Other channels (EKG, EOG)
2. Is there normal brain activity or is it altered? • Is the stuff that is supposed to be there actually there ? • Is there evidence of a structural lesion or a toxic/metabolic process that has altered the normal EEG background activity?
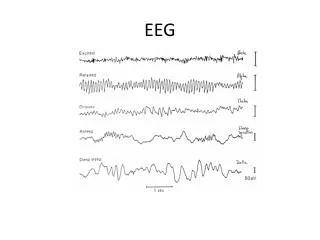
Normal brain activity • Waves: Delta 1-3 Hz Theta 4-7 Hz Alpha 8-12 Hz Beta > 12 Hz • Posterior dominant alpha rhythm with eye closure. • Alpha rhythm ≠ alpha frequency • Low amplitude, frontal Beta activity.
Normal deviations from normal (!) • Drowsiness • Sleep • Age (young and old!) • Activation procedures (a) Hyperventilation (b) Photic stimulation
Background abnormalities • Slowing (theta or delta) • Focal or diffuse • Bilaterally synchronous or not • Rhythmic vs. irregular/polymorphic • High vs. low amplitude • Intermittent vs. continuous • Can be more subtle • Attenuation of amplitude • Asymmetry of alpha Etc…
Summary • Focal slowing = rule out structural lesion • Generalized rhythmic slowing = consider deep structural lesion or destructive process • Polymorphic generalized slowing = very nonspecific “Disturbance of the background activity”
3. Abnormal activity Is there any stuff there that should not be there at all ? Not simply alteration of the background Usually, we are asking if there is epileptic activity (interictal or ictal).
Focal Inter-ictal activity • Spikes and sharp waves ! • Phase reversal • Recurrent and consistent • With a field • Followed by slow wave • Asymmetrical • Not explained by artifact
Terminology “Potentially epileptic abnormality” “Epileptiform abnormality”
Generalized Inter-ictal Activity Generalized spike and wave
Ictal Activity (Seizures) • Electrographic lasts > 10 sec • Seizures not defined by single pattern; spikes, spike and wave, slowing, attenuation etc… • Rhythmic activity that changes with time
Summary • Interictal epileptic activity = spikes and sharp waves • Ictal epileptic activity = evolving rhythmic activity
4. State • 4 Sleep stages, plus REM 1. Lose α, slow EOM, v-waves 2. Spindles, K-complex, v-waves 3. Delta < 50% 4. Delta > 50% REM: -looks normal (i.e. awake), need EOG, EMG etc… • Sleep onset • Most consider stage 1 sleep = drowsiness • But…some define sleep onset as appearance of v-waves, others as sleep spindles.
Don’t Forget… 5. Age • Prior to birth, continuous evolution of EEG • Posterior-dominant rhythm by 6-12 months; alpha frequency by 4-8 years 6. Artifacts • EKG or pulse • Eye movement • Electrode • Muscle/movement • Electrical • Weird and wonderful
So how do you read an EEG? “Plan and scan” Organized Approach Orient Normal Abnormal Age and State Artifacts Scanning Vertical Horizontal
If all else fails… Describe what you see From Fisch and Spehlmann