Download
1 / 1
10 likes | 189 Vues
Effect of Successfully Completing a HIV Treatment Adherence Program on Participant Hospital Admissions at a New York State Suburban Hospital`. H. Pahlevan-Sabbagh , G. Feleke, J. Verley. THPE0134. Result. Diagram 1.

E N D
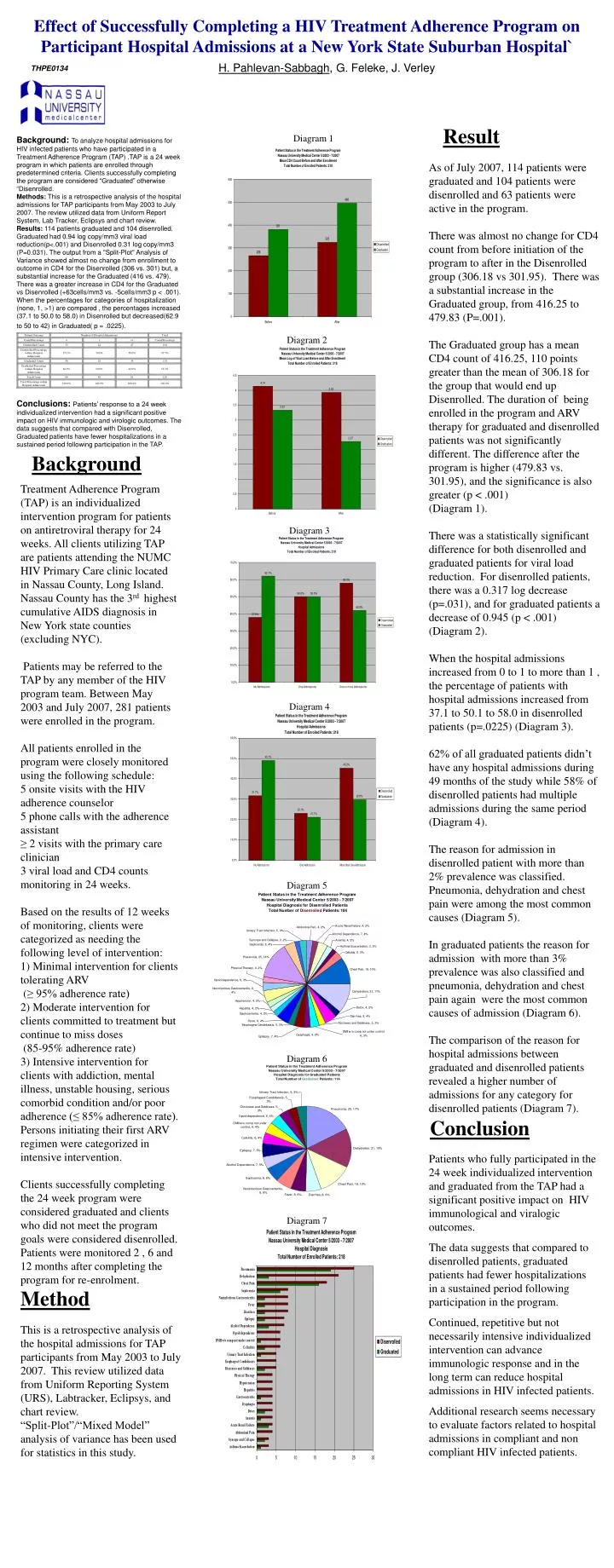
Effect of Successfully Completing a HIV Treatment Adherence Program on Participant Hospital Admissions at a New York State Suburban Hospital` H. Pahlevan-Sabbagh, G. Feleke, J. Verley THPE0134 Result Diagram 1 Background: To analyze hospital admissions for HIV infected patients who have participated in a Treatment Adherence Program (TAP) .TAP is a 24 week program in which patients are enrolled through predetermined criteria. Clients successfully completing the program are considered “Graduated” otherwise “Disenrolled. Methods: This is a retrospective analysis of the hospital admissions for TAP participants from May 2003 to July 2007. The review utilized data from Uniform Report System, Lab Tracker, Eclipsys and chart review. Results: 114 patients graduated and 104 disenrolled. Graduated had 0.94 log copy/mm3 viral load reduction(p<.001) and Disenrolled 0.31 log copy/mm3 (P=0.031). The output from a "Split-Plot" Analysis of Variance showed almost no change from enrollment to outcome in CD4 for the Disenrolled (306 vs. 301) but, a substantial increase for the Graduated (416 vs. 479). There was a greater increase in CD4 for the Graduated vs Disenrolled (+63cells/mm3 vs. -5cells/mm3 p < .001). When the percentages for categories of hospitalization (none, 1, >1) are compared , the percentages increased (37.1 to 50.0 to 58.0) in Disenrolled but decreased(62.9 to 50 to 42) in Graduated( p = .0225). Conclusions: Patients’ response to a 24 week individualized intervention had a significant positive impact on HIV immunologic and virologic outcomes. The data suggests that compared with Disenrolled, Graduated patients have fewer hospitalizations in a sustained period following participation in the TAP. As of July 2007, 114 patients were graduated and 104 patients were disenrolled and 63 patients were active in the program. There was almost no change for CD4 count from before initiation of the program to after in the Disenrolled group (306.18 vs 301.95). There was a substantial increase in the Graduated group, from 416.25 to 479.83 (P=.001). The Graduated group has a mean CD4 count of 416.25, 110 points greater than the mean of 306.18 for the group that would end up Disenrolled. The duration of being enrolled in the program and ARV therapy for graduated and disenrolled patients was not significantly different. The difference after the program is higher (479.83 vs. 301.95), and the significance is also greater (p < .001) (Diagram 1). There was a statistically significant difference for both disenrolled and graduated patients for viral load reduction. For disenrolled patients, there was a 0.317 log decrease (p=.031), and for graduated patients a decrease of 0.945 (p < .001) (Diagram 2). When the hospital admissions increased from 0 to 1 to more than 1 , the percentage of patients with hospital admissions increased from 37.1 to 50.1 to 58.0 in disenrolled patients (p=.0225) (Diagram 3). 62% of all graduated patients didn’t have any hospital admissions during 49 months of the study while 58% of disenrolled patients had multiple admissions during the same period (Diagram 4). The reason for admission in disenrolled patient with more than 2% prevalence was classified. Pneumonia, dehydration and chest pain were among the most common causes (Diagram 5). In graduated patients the reason for admission with more than 3% prevalence was also classified and pneumonia, dehydration and chest pain again were the most common causes of admission (Diagram 6). The comparison of the reason for hospital admissions between graduated and disenrolled patients revealed a higher number of admissions for any category for disenrolled patients (Diagram 7). Diagram 2 Background Treatment Adherence Program (TAP) is an individualized intervention program for patients on antiretroviral therapy for 24 weeks. All clients utilizing TAP are patients attending the NUMC HIV Primary Care clinic located in Nassau County, Long Island. Nassau County has the 3rd highest cumulative AIDS diagnosis in New York state counties (excluding NYC). Patients may be referred to the TAP by any member of the HIV program team. Between May 2003 and July 2007, 281 patients were enrolled in the program. All patients enrolled in the program were closely monitored using the following schedule: 5 onsite visits with the HIV adherence counselor 5 phone calls with the adherence assistant ≥ 2 visits with the primary care clinician 3 viral load and CD4 counts monitoring in 24 weeks. Based on the results of 12 weeks of monitoring, clients were categorized as needing the following level of intervention: 1) Minimal intervention for clients tolerating ARV (≥ 95% adherence rate) 2) Moderate intervention for clients committed to treatment but continue to miss doses (85-95% adherence rate) 3) Intensive intervention for clients with addiction, mental illness, unstable housing, serious comorbid condition and/or poor adherence (≤ 85% adherence rate). Persons initiating their first ARV regimen were categorized in intensive intervention. Clients successfully completing the 24 week program were considered graduated and clients who did not meet the program goals were considered disenrolled. Patients were monitored 2 , 6 and 12 months after completing the program for re-enrolment. Diagram 3 Diagram 4 Diagram 5 Diagram 6 Conclusion Patients who fully participated in the 24 week individualized intervention and graduated from the TAP had a significant positive impact on HIV immunological and viralogic outcomes. The data suggests that compared to disenrolled patients, graduated patients had fewer hospitalizations in a sustained period following participation in the program. Continued, repetitive but not necessarily intensive individualized intervention can advance immunologic response and in the long term can reduce hospital admissions in HIV infected patients. Additional research seems necessary to evaluate factors related to hospital admissions in compliant and non compliant HIV infected patients. Diagram 7 Method This is a retrospective analysis of the hospital admissions for TAP participants from May 2003 to July 2007. This review utilized data from Uniform Reporting System (URS), Labtracker, Eclipsys, and chart review. “Split-Plot”/“Mixed Model” analysis of variance has been used for statistics in this study.