Download
1 / 101
1.87k likes | 3.32k Vues
Peripheral IV Insertion with Ultrasound Guidance. Education Requirements. Anatomy and physiology limbs, to include vein, artery, and nerves Assessment of vessels Appropriate vessels and cannulation techniques Pain management Aseptic technique Appropriate length and size of needles

E N D
Education Requirements • Anatomy and physiology limbs, to include vein, artery, and nerves • Assessment of vessels • Appropriate vessels and cannulation techniques • Pain management • Aseptic technique • Appropriate length and size of needles • Complications, management, and troubleshooting • Management of patient • Machine operation, role of gel • Cleaning machine between patients
Vein Composition • Inner layer - tunica intima • Smooth elastic endothelial lining facilitates blood flow • Valves are formed by fold in endothelium • Easily disturbed by venipuncture, catheter advancement, activity during catheter dwell • Damage to endothelial lining may initiate inflammatory response
Vein Composition • Middle layer - tunica media • Smooth muscle and fibrous tissue arranged around circumference of vessel • Thickest layer • Patient anxiety, hypothermic events, and mechanical/chemical irritation can stimulate nerve fibers resulting in venospasm
Vein Composition • Outer layer - tunica adventitia • Connective tissue - provides support and protection for vein • Contains microcirculation that provides nutrients • Includes innervation by nerve fibers which control vasoconstriction and vasodilation
Structural Differences Tunica Intima • Arteries • thin to allow for diffusion of metabolites • Capillaries • single layer of endothelium and thin basal lamina • Veins • endothelial layer of shorter, broader cells and basal lamina
Structural Differences Tunica Media • Arteries • smooth muscle fibers controlling constriction and relaxation • Capillaries • no middle layer • Veins • elastin fibers and smooth muscle fibers, thinner than same layer in arteries
Structural Differences Tunica Adventitia • Arteries • contain collagen and elastin • contain efferent and afferent nerve fibers • Capillaries • thin reticular tissue with occasional fibroblasts and mast cells • Veins • loose connective tissue with elastin fibers
Vascular Distensibility • Venous walls can distend 6 - 10 times more than arterial walls • Small increase in pressure results in much larger quantity of blood • 3 times more blood volume on the venous side than the arterial side
Stress-Relaxation Phenomenon Post-Tourniquet Application • Smooth muscle fibers in vein elongate to accommodate the increased blood volume • Pressure increases quickly, then resumes normal levels with increased blood volume • Volume and pressure fall when tourniquet removed, but are soon reestablished • Advancement of catheter before process complete may result in pathway resistance
Patient Centered Considerations • Patient desires for left or right arm use • Known arm and chest complications • Other implanted devices • Current risk factors to use of either arm • Abnormalities in anatomical size and/ or condition of specific veins based on ultrasound assessment (without a tourniquet) • Selection of the largest vein suitable for the size of IV necessary to accomplish clinical needs of infusion, blood sampling, contrast injection.
Patient Centered Considerations Patient desires for left or right arm use Known arm and chest complications Other implanted devices Current risk factors to use of either arm Abnormalities in anatomical size and/ or condition of specific veins based on ultrasound assessment (without a tourniquet) Selection of the largest vein suitable for the size of IV necessary to accomplish clinical needs of infusion, blood sampling, contrast injection.
Vein Assessment with Ultrasound Tourniquets are placed above the intended insertion site and are applied to impede venous flow, but not arterial flow Place on upper part of the extremity so that the entire vessel can be assessed for vessel patency. It is recommended that vessels be 2 times the outer diameter of the catheter without a tourniquet so that blood flows around the catheter.
Vein Selection Assess entire extremity for signs of Phlebitis, infiltration, extravasation Dermatologic conditions Surgery or accidents which may have altered normal venous pathways Dialysis grafts/fistulas
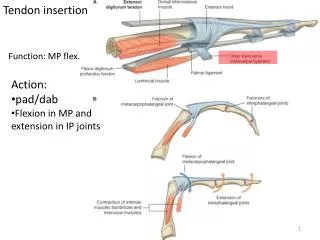
Median Cubital Sites for children and/or adults without ultrasound access communicates directly with basilic vein presents medially well-supported by biceps brachial tendon commonly used for peripheral catheter insertion and lab draws
Adding Venous Ultrasound To Vascular Access Represents a Technique Change: Different positioning of the arm Accessing vessels above the antecubitalfossa Visualizing the screen and not the insertion site for venipuncture Holding the probe in one hand and accessing the vein with the other This requires an adjustment to new visual focus using instrumental guidance.
Advantages of Ultrasound GuidedVAD placement Enhances vein selection Aides critical thinking Lower complication rates Decreases attempts at venipuncture Prevents damage to surrounding structures Prevents delays Increased patient satisfaction
What is Ultrasound? Ultrasound is cyclic sound pressure with a frequency greater than the upper limit of humanhearing. The production of ultrasound is used in many different fields, typically to penetrate a medium and measure the reflection signature
How does ultrasound work? The handheld transducer or “probe” contains 300 piezoelectric crystals that vibrate in response to electrical signals received through the cable
How does ultrasound work? The crystal vibration produces sound waves that pass through the body. Tissues reflect or “echo” sound waves back to the probe The sound waves are then translated back into electrical signals and sent to the CPU in the ultrasound unit.
How does ultrasound work? The computer creates grayscale images of the underlying structures. Fluid filled spaces appear dark Denser structures become white Brightness depends on the strength of the returning signal Ultrasound cannot penetrate air or bone. Bone – very dark Tissue – whites and grays
Machine Controls Depth of field: magnifies the image Gain increases or decreases amplitude “amplifies the signal” magnifies image details Orientation marker System presets
Assessment Equipment Ultrasound gel is necessary for conduction of sound waves Warm gel prevents vasoconstriction Bactericidal wipe Gloves
Assessment Systematic approach Explain procedure Darken room Provide warm environment Position patient for comfort Obtain patient history CVA Pacemaker or AICD Thrombus Previous surgery CVAD placement Assess skin integrity
What characteristics do I need to assess? ASSESSMENT Flow Shape Patency Path Size NORMAL FINDINGS Normal venous flow on color pulse doppler Flow increases with augmentation Regular lumen shape and size Compressible Non tortuous path No evidence of echogenic material within the lumen
Probesmanship Sliding Rocking Angling Rotating Use non-dominant hand to maneuver probe Use dominant hand for venipuncture
The Probe Place the probe against the skin Hold the probe so the needle guide notch points towards the inserter Center the marker on the target vessel
Technique Holding the probe at 90 degrees and needle at 20-45 degrees. Once the puncture is through the skin all attention is turned to the ultrasound screen. 90 45 Vein Vein
Needle pushing on vein Note the vein starting to dimple in and the bevel of the needle.
Orientation What you see on the Screen is the same as you would see if you could see a vertical plane through the patient’s arm. Patient’s Arm L R As you look at the arm. Your Left and Right. Screen
Depth Markers The US screen shows white marks running down the center of the screen Each white mark represents a specified distance In 2cm Mode
Vascular Assessment Suitable veins and their approximate size. How deep is the vein? Is the vein narrowed or occluded? Is the vein path straight or tortuous? Are there obstructions or confluence? Is the vein next to an artery? Does the vein narrow further up the arm? (stenosis)
Transducer Orientation Transverse plane Cross sectional view Veins and arteries appear as circles Light borders and dark centers Most common view used by nurses Allows visualization of surrounding structures Sagittal plane Veins appear as long tubes View commonly used by physicians Allows for better visualization of needle tip as it approaches the vein Unable to view surrounding structures
Vein Appearance in Both planes Transverse View Sagittal View (Longitudinal) Valve
Nerve Identification Brachial nerves
Brachial vein Brachial nerve complex Brachial artery Brachial vein
Brachial Nerve Identification Brachial nerve
Brachial Vein and Artery Basilic vein is up over here V A
Thrombosed Vein Appearance on Ultrasound Diminished flow with augmentation Presence of multiple collateral vessels Loss of compressibility Older thrombi appear more echogenic Vessels shrink with chronic thrombosis New thrombi will appear softly echogenic Valve cusps are particularly vulnerable to thrombus formation