Download
1 / 23
270 likes | 638 Vues
Anti-ganglioside antibodies. The cause of otherwise unexplained ophthalmoplegias? Michelle Gajus and Lionel Kowal. Antiganglioside antibodies are responsible for some autoimmune diseases. Antiganglioside antibody. ANTI Gq1b. Acute conditions Miller-Fisher Syndrome Acute ophthalmoparesis

E N D
Anti-ganglioside antibodies The cause of otherwise unexplained ophthalmoplegias? Michelle Gajus and Lionel Kowal
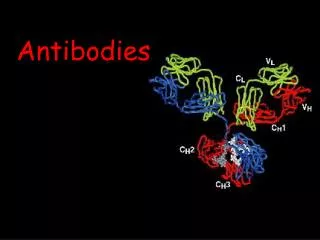
Antiganglioside antibodies are responsible for some autoimmune diseases Antiganglioside antibody
ANTI Gq1b • Acute conditions • Miller-Fisher Syndrome • Acute ophthalmoparesis (ophthalmoplegia without ataxia) • Chronic conditions • Otherwise unexplained ophthalmoplegia Chronic ophthalmoplegia with anti-GQ1b antibody. Reddel et alii Neurology. 54(4):1000-2, Feb 2000 & some Japanese papers
ANTI GM-1 • Guillain-Barre syndrome • Multifocal motor neuropathy • Distal lower motor neuron syndrome • McCombe: Asymmetric patchy muscle weakness
Five cases of anti GM-1 [normal anti-GQ1b] in ophthalmoplegia of obscure cause
EG - 13 y female • ‘Acute’ ET • Intermittent at first • No strabismogenic factors present • 50^ 70^ ET in one month • BMR + botox : good result
SN - 31 y female • Ptosis surgery as a child • 3 years of intermittent LXT • Other examination normal
SN - 31 y female • LMR Rs 10 mm to slightly restrict abduction, • LLR Rc to LIO insertion • Cosmesis OK; no diplopia
JL - 50 y male • Previously well; No HT, DM • Sudden onset R vertical diplopia • Impaired depression RE; excyclo RE • ‘ R SOP of indeterminate cause ‘ • No treatment • Symptoms completely resolved over 5 mo
LK - 58 male • No HT, DM • ‘Shimmering’ visual disturbance followed by diplopia • H&V diplopia esp. down left gaze • Exotropia on L gaze • Provisional diagnosis R CN IV • All resolved in 2 months
JP - 67 female • Past history of well-controlled hypertension • 4 months of intermittent diplopia on L gaze • With glasses 6^ ET, with CL 1^ • Orthophoric in primary position • 1^ fusional divergence, 26^ of fusional convergence • Normal ocular rotation,V1, pupillary reaction, MRI • No abduction deficit • Diagnosis: subtle L VI with no localising signs • No treatment
Nomenclature • ‘Ganglioside’: lipids from ganglion cells of brain (Klenk ‘42) • Oligoglycosylceramides with sialic acid residues joined to the monosaccharide units. • Short-hand nomenclature system: M, D, T, Q = mono-, di- ,tri- & quatro- sialog-sides hence GQ, GM • 1, 2, 3, etc refer to the order of migration of the g-sides on thin-layer chromatography. Order of migration of monos/g-sides is GM3 > GM2 > GM1 • To indicate variations within the basic structures, further subscripts are added, e.g. GM1a, GD1b.
Distribution of anti-GQ1b • GQ1b g-sides are clustered in paranodal region of human ocular motor nerves • Paranodal region: • - important for nerve conduction • - not protected by blood brain barrier or by connective tissue sheaths of the peripheral nerves. • GQ1b Ab’s can easily target these vulnerable sites.
Distribution of GQ1b Other cranial and peripheral nerves
Anti-GM1 • III, IV,VI : more GQ1b g-sides cf other cranial nn • propensity for ophthalmoplegia with GQ1b Ab’s. • Concentration of GM1 g-sides in ocular motor nerves no higher than other cranial nn. • mechanismof action of Ab’s against GM1 less clear than for GQ1b
Anti-GM1 • In about 20 consecutive cases of acquired ophthalmoplegia of obscure cause: 5 positive cases for anti-GM1. • Our finding suggests that they may play a part in some otherwise unexplained ophthalmoplegia. • Pathogenesis yet to be elucidated.