Bullous diseases
Bullous diseases. Vesicles and bullae are accumulations of fluid within or under the epidermis. Subepidermal blisters Occur between the dermis and the epidermis. Their roofs are relatively thick and so they tend to be tense and intact. They may contain blood. Intra-epidermal


Bullous diseases
E N D
Presentation Transcript
Vesicles and bullae are accumulations of fluid within or under the epidermis. • Subepidermal blisters • Occur between the dermis and the epidermis. • Their roofs are relatively thick and so they tend to be tense and intact. • They may contain blood. • Intra-epidermal • blisters appear within the spinosum cell layer of the epidermis • So have thin roofs and rupture easily • Leave an oozing denuded surface.
Subcorneal blisters • Form just beneath the stratum corneum at the outermost edge of the epidermis • Have even thinner roofs • Tendency to break is more marked
Classification*** • Bullous Pemphigoid • Bullous Pemphigoid • Chronic Bullous Disease of Childhood • Cicatricial Pemphigoid • Epidermolysis Bullosa Acquisita • Linear IgA Dermatosis • Pemphigoid • Pemphigus • Pemphigus • Pemphigus Foliaceus • Pemphigus Vegetans • Pemphigus Vulgaris
pemphigus pemphigoid • Age:middle aged • Clinical features: monomorphic • Blisters: flaccid,ruptures easily • Content of blisters: fluid filled. • Oral lesion :are common • Nikolsky’s sign:Positive • Tzank smear:acantholytic cells are seen • Elderly • Polymorphic • Tense ,firm • Mostly hemmorhagic • Less common • Negative • No acantolytic cells.
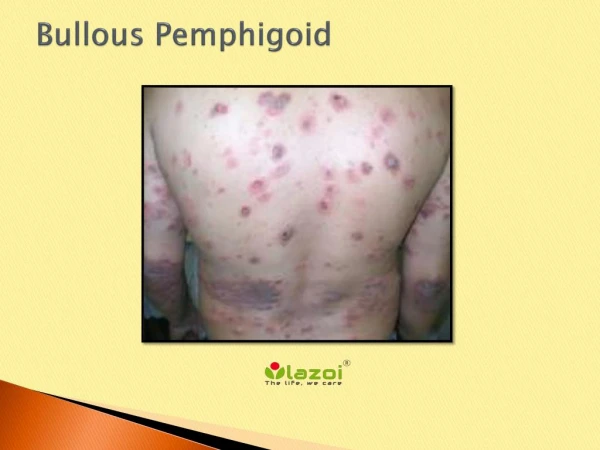
Bullous Pemphigoid • It is an autoimmune disorder, meaning it is caused when the body's immune system malfunctions. • The immune system is meant to defend the body against bacteria, viruses, and disease, but instead produces antibodies against healthy tissue, cells and organs. • Some patients with BP have other diseases such diabetes and rheumatoid arthritis. • Other factors triggering BP include drugs (Furosemide, penicillin), mechanical trauma, and physical traumas (burns from radiation, sun or heat)
Bullous Pemphigoid*** • Epidemiology • Age of onset- elderly • Men and women affected equally • Pathophysiology • Autoimmune Subepidermal Blistering • Symptoms • Pruritus • Lesions may be tender at borders • Signs • Initial Urticarial eruption • Develops into large tense bullae after weeks to months • Contain clear fluid or may at times be hemorrhagic • Diffuse cutaneous involvement • Often involves lower legs, forearms, thighs, groin • Also involves abdomen • Mucosa much less affected than in pemphigous vulgaris • No scar formation • Milia formation as lesion heals
Labs • Histology • Supepidermal Blister • Superficial dermal inflammation • Immunofluorescence • Ig G and C3 deposition along basement membrane zone • Management • First-Line • Prednisone • Methotrexate may be used for prednisone intolerance • Topical corticosteroids in localized mild cases • Adjunctive agents • Azathioprine • Mycophenolate mofeti • Tetracycline • Course • Self-limited condition • Remits with treatment by 6 years in 50 % of cases
Chronic Bullous disease of childhood • Epidemiology • Age of Onset: Under age 5 years • Pathophysiology • Autoimmune bullous disorder • Variant of Linear IgA Dermatosis (seen in adults) • Symptoms • Pruritus and burning sensation • Signs • Tense inflamed Blisters over red base • May appear as collarettes of Blisters • Distribution • Most commonly found on genitalia • Also may involves face and perioral skin • Oral Mucosa involved in 50% of cases
Course • Resolves within 2 years of onset in most cases Histology • Subepidermal Blisters • Inflammatory infiltrates at basement membrane zone Immunofluorescence • IgA deposition along basement membrane • Management • First Line: Dapsone or Sulfapyridine • (requires G6PD and monitoring of CBC) • Adjunct: Low dose prednisone initially
Cicatricial Pemphigoid *** Epidemiology • Incidence (rare): 1 in 12,000 to 20,000 • Ages affected: 60 to 80 years • Gender predominance: Women by male ratio of 2:1 • Pathophysiology • Autoimmune bullous condition • Associated conditions • Stevens-Johnson Syndrome • Medications • Topical Glaucoma medications • Practolol • Clonidine • Signs • Blistering of mucus membranes • Blister ruptures within hours of formation • Painful Erosion
Most Erosions heal without scarring • Most common sites of involvement • Oral Mucosa (most often buccal and palatal mucosa) • Results in erosive Gingivitis • Conjunctiva (usually bilateral) • Results in chronic Conjunctivitis and scarring • Other sites of involvement • Skin (usually non-scarring) • Scalp (Cicatricial Alopecia) • Pharynx and larynx • External genitalia • Nasal mucosa • Anus • Esophagus
Labs: Histology • Subepidermal bulla • Perivascular inflammatory cell infiltrates • Fibrosis distinguishes from Bullous Pemphigoid • Immunofluorescence with IgG, C3, IgA deposits • Forms linear band at Basement Membrane Zone • Differential Diagnosis • Bullous Pemphigoid • Epidermolysis Bullosa Acquisita(EBA) • Linear IgA Bullous Dermatosis(LABD) • Systemic Lupus Erythematosus • Pseudopemphigoid • Pemphigus
Management: • Early aggressive treatment • First-Line: Prednisone 0.5 to 0.75 mg/kg/day x6 months • Ocular Involvement: Azathioprine or Cyclophosphamide • Skin Involvement: Topical Corticosteroids • Oral Involvement • Dapsone • Corticosteroid gel • Dexamethasone mouthwash • Complications • Ocular Lesions may result in blindness • Laryngeal stricture • Esophageal Stricture • Supraglottic Stenosis
Epidermolysis Bullosa Acquisita** • Epidemiology • Mean age of onset: 50 years • Few isolated cases of children seen • Pathophysiology • Autoimmune Subepidermal Blistering condition • Signs • Trauma prone areas more commonly affected • Tense Blisters and Erosions over extensor surfaces • Knuckles • Dorsal hands • Elbows • Knees • Ankles • Mucosal involvement • Oral, nasal, and esophageal mucosa • Conjunctival mucosa
classification • Simple Epidermolysis bullosa • Junctional Epidermolysis bullosa • Dystrophic Epidermolysis bullosa • Acquired Epidermolysis bullosa
Dystrophic Epidermolysis bullosa
Linear IgA Dermatosis • Epidemiology • Onset over age 30 years • Pathophysiology • IgA mediated dermatosis mediated by IgA and causes "sausage-like" lobulated blisters arranged at the outer edges of flattened erythematous patches. • Autoimmune bullous disorder • Variant of Chronic Bullous Disease of Childhood
Symptoms • Pruritus • Signs • Annular Lesions • Papules (may be excoriated and crusted) • Vesicles • Bullae • Distribution • Symmetric involvement on extensor surfaces • Elbows, knees, and buttocks affected • Mucosa involvement may occur (Conjunctiva, oral)
Labs • Histology • Subepidermal Blister with inflammatory infiltrate • Immunofluorescence • IgG deposits at dermal-epidermal junction • Complications • Scarring skin lesions (with associated Milia) • Differential Diagnosis • Porphyria cutanea tarda • Hereditary Epidermolysis bullosa • Bullous Pemphigoid Course • Chronic waxing and waning course