Download
1 / 45
490 likes | 893 Vues
Endometriosis & Adenomyosis. Zhao aimin M.D., Ph.D., Professor Department Of Obstetrics & Gynecology

E N D
Endometriosis & Adenomyosis Zhao aiminM.D., Ph.D., Professor Department Of Obstetrics & Gynecology Renji Hospital Affiliated to SJTU School of Medicine
Definition: Abnormal growth of endometrial tissue outside the uterine cavity.
Incidence and Prevalence: • Increase significantly • Range from 1~50% General population:1~2% Infertile women:30~50% • Occurs primarily in women in 25~45s
Pathogenesis: • Implantation Theory Retrograde Menustration Theory Sampson,1921 • Lymphatic and Vascular Dissemination Theory Javert,1952 • Coelomic Theory Meyer • Genetic Theory • Immune System Dysfunction(immunologic theory)
Genetic factors: • Familial clustering of endometriosis is a common clinical observation. • In families with endometriosis,the disease is often confined to the maternal line,and is 7 times more common in first-degree relatives than in the general population. • In future studies,evaluation of DNA polymorphism may identify specific genes involved in the development of endometriosis.
Immunologic Theory: • Lose control of immunologic balance • Both cellular immunity and humoral immunity change. • Macrophage↑ release IL–1、IL–6、TNF、EGF、FGF etc. stimulate T、B lymphocyte proliferation and activation • Activity of killer cell(NK cell and T cell)↓ • Produce anti–endometrium antibody • Abnormal expression of CAMs(cell adhesion molecules)
The pathogenesis is unclear. • multifactor
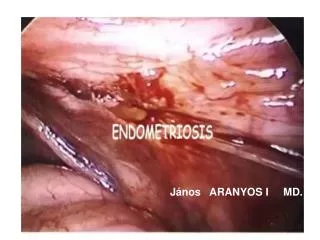
Pathology–macroscopic appearance(1): • The commonest sites: • Ovary(chocolate cyst) • Peritoneum of the recto–vaginal cul–de–sac of the Pouch of Douglas • Utero–sacral ligaments • Sigmoid colon • Broad ligament
This is a section through an enlarnged 12 cm ovary to demonstrate a cystic cavity filled with old blood typical for endometriosis with formation of an endometriotic, or "chocolate", cyst.
Pathology– macroscopic appearance (2): • Less common sites: • Cervix • Round ligament • Urinary system(bladder、ureter) • Umbilicus • Appendix • Laparotomy scars
Multiple appearances ofendometriosisimplants: • Brownish,discolored peritoneum • Superficial peritoneal ecchymosis • Raised,reddish,superficial nodules • Reddish–blue invasive nodules • Fibrotic,whitish nodules • Raised,glossy,translucent blobs • Patchy,white opacified peritoneum • Reddish or bluish ovarian cysts
Grossly, in areas of endometriosis the blood is darker and gives the small foci of endometriosis the gross appearance of "powder burns". Small foci are seen here just under the serosa of the posterior uterus in the pouch of Douglas. Such areas of endometriosis can be seen and obliterated by cauterization via laparoscopy.
Upon closer view, these five small areas of endometriosis have a reddish-brown to bluish appearance.
Pathology– microscopic appearance • Histomorphologically similar to eutopic endometrium • Four major components: endometrial glands endometrial stroma fibrosis hemorrhage Eutopic endometrium 在位子宫内膜 Ectopic endometrium 异位子宫内膜
Symptoms: • Pain progressive dysmenorrhea dyspareunia painful defecation • Menstrual disturbance • infertility dysmenorrhea 痛经 dyspareunia 性交痛
Signs: • Enlargement of the ovaries,fixed • Fixed retroversion of the uterus • Tender nodules within the pelvis • Cannot be diagnosed by PV alone. • Should always be considered when patients have symptoms referable to the pelvic cavity.
Very variable • Vary with the focus location • Often bear no relation to the extent of the disease • Quite often deposits are found incidentally in women who have no symptoms. (25% have no symptoms)
Diagnosis: • History • PV examination • Laparoscopy(golden standard) • Ultrasonography(B–type ultrasound) • CA–125↑(<200U/ml;normal value 35U/ml) • Anti–endometrium antibody(+)
Staging systems: • In the AFS-r(1985)staging system,points are assigned for severity of endometriosis based on the size and depth of the implant and for the severity of adhesions. • The points are summed and the patients are assigned to one to four stages: Stage I —minimal disease, 1~5 points Stage II — mild disease, 6~15 points Stage III — moderate disease,16~40 points Stage IV — severe disease, ≥40 points
Differential diagnosis: • Malignant ovary tumours • Pelvic inflammatory masses • Adenomyosis
Expectant therapy: • Indications:with very limited disease (whose symptoms are minimal or nonexistent) • If trying to get pregnant,the best way is to accept laparoscopic therapy as early as possible.
Medical therapy: • Indications:chronic pelvic pain severe dysmenorrhea no require to get pregnant no ovarian cyst formation • Hormone–inhibition therapy
Drugs: • Danazol:pseudomenopause therapy • Gestrinone • GnRH – a:medical oophorectomy add – back therapy • Mifepristone RU486 • Progestogens:pseudopregnancy therapy
Surgical therapy(1): • Indications(1)adnexal mass (2)pelvic pain (3)infertility • Approaches: (1) trans – abdominal (2) laparoscopic
Surgical therapy(2): Methods: • Conservative surgery • preserve the fecundity • preserve the ovarian function • Definitive surgery: hysterectomy + salpingo–oophorectomy
Combination medical–surgical treatment: Three–step: surgery medical therapy second look(laparoscopy)
It is important to individualize the choice of therapy. • Therapy must be tailored to • the degree of symptomatology • the patient’s age • her desire to maintain fertility
Prognosis: • With proper treatment,the prognosis is good for relief of pain and enhancement of fertility in mild to moderate endometriosis. • In most cases,hormonal therapy is temporarily effective in controlling symptoms and arresting growth but is generally less effective than surgery in increasing fertility. • The recurrent rate is very high.
Prevention: • Avoid possible augmentation of menstrual reflux. • Taking oral contraceptive is recommended. • Isolation and irrigation of the operative site.
Criticalpoints(1): • The pathogenesis is poorly understood,but emerging evidence supports the causative role of retrograde menstruation and implantation of endometrial tissue. • Endometriosis is a common in women with pelvic pain or infertility. • Laparoscopy is the optimal technique to diagnose pelvic endometriosis.
Criticalpoints(2): • In most cases,surgical therapy at the time of initial diagnosis effectively relieves pain and may enhance fertility. • Alternatively,medical therapy with progestins、danazol、gestrinone or GnRH-a will ameliorate pelvic pain,but they do not enhance fertility. • Endometriosis is a recurrent disease,and definitive treatment with removal of pelvic organs may be necessary.
Definition: A benign uterine condition in which endometrial glands and stroma are found deep in the myometrium.
Etiology: • Basal endometrial hyperplasia invading a hyperplastic myometrial stroma. • Four primary theories: • Heredity • Trauma • Hyperestrogenemia • Viral transmission
Pathology — gross appearance: • Usually hyperemic with thickened walls • The foci are frequently scattered diffusely throughout the myometrium. • Occasionally,may be more circumscribed,with the formation of a distinct nodule,an adenomyoma. Adenomyosis 子宫肌腺症 Adenomyoma 子宫肌腺瘤
The thickened and spongy appearing myometrial wall of this sectioned uterus is typical of adenomyosis. There is also a small white leiomyoma at the lower left.
Clinical features(1): • Symptomatic adenomyosis occurs primarily in parous women over the age of 40 . (30~50) • Classic symptoms: secondary dysmenorrhea abnormal uterine bleeding
Clinical features(2): • Most common physical sign: a diffuselyenlarged uterus , (rarely exceeds 12 weeks’ gestation in size) particularly tender during menstruation
Diagnosis: • History • Pelvic examinations • Ultrasonography • Serum markers:CA-125↑
Treatment: • Hormone therapy • Hysterectomy,the only uniformly successful treatment for adenomyosis,is necessary.
Thanks for Your Attention Zhao aiminM.D., Ph.D., Professor Department of Obstetrics & Gynecology Renji Hospital Affiliated to SJTU School of Medicine