Module 8: TB Recording and Reporting
750 likes | 947 Vues
Module 8: TB Recording and Reporting. Learning Objectives. Define surveillance Accurately complete the orange Tuberculosis Treatment Card Accurately complete the TB register Explain the flow of TB data from the health facilities up to the national level. What is Surveillance?.

Module 8: TB Recording and Reporting
E N D
Presentation Transcript
Learning Objectives • Define surveillance • Accurately complete the orange Tuberculosis Treatment Card • Accurately complete the TB register • Explain the flow of TB data from the health facilities up to the national level
What is Surveillance? • The ongoing, systematic collection, analysis, interpretation, and reporting of health-related data • Data can be used to plan, implement, and evaluate public health programmes aimed at preventing disease and improving life
Examples of Surveillance Activities • TB recording and reporting systems • HIV antenatal sentinel surveillance • Tracking HIV positive patients on ARVs • Other disease surveillance activities (e.g. malaria)
What is TB/HIV Surveillance? It has two components: • Recording and reporting of TB information (smear status, anti-TB treatment, TB treatment outcomes) • Recording and reporting of HIV data (HIV status, ART use, IPT history) for TB patients
TB Surveillance Data Collection of routine TB/HIV data will serve to: • Promote information sharing • Understand the TB/HIV epidemic and its effect on patients and communities • Direct resources and planning • Evaluate the impact of interventions
TB RECORDING AND REPORTING (R&R) • Is one offive components of Directly Observed Treatment Strategy (DOTS) • Provides data for patient care, national surveillance, evaluation of programs • WHO, IUATLD have standardised forms for TB R&R • Paper-based, electronic, or a combination of both
BOTSWANA TB R&R Forms • TB Suspect and Sputum Dispatch Register • Mycobacteriology Request Form • Laboratory TB Register • Health facility TB Register • Contact Form • OrangeTuberculosis Treatment Card • Blue patient appointment and DOT card • District TB Register • Electronic TB Register (ETR) • Transfer of Patient
Data TB suspect provides 3 sputum specimens HCW enters patient data in the TB suspect register Health facility HCW enters patient data on the orange treatment card and into facility TB register Data from facility TB register copied into district TB register by District TB Coordinator Data entered into Electronic TB register (ETR) by District TB Coordinator District TB coordinator uses ETR to generate quarterly cohort and yearly reports District TB coordinator saves data to a floppy disk and sends to the national level District District-level data are collated in the ETR for analysis at the national level BNTP generates quarterly and yearly reports for the district- and country-levels using ETR National FLOW OF DATA THROUGH THE NATIONAL TB PROGRAM
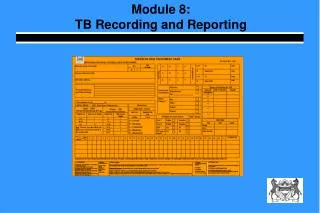
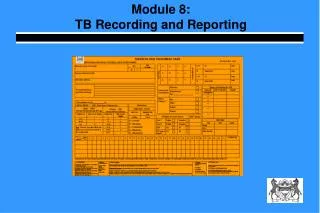
ORANGETB TREATMENT CARD • Initial source of data for the TB recording and reporting system • Pink cards NOT TO BE USED • Diagnosis and treatment information • Should be completed by MDs and nurses • Information from the treatment card is used to fill in the facility and district TB registers • Information should be complete and accurate • SOME data is better than NO data !!
Name (Surname, First Name) • How to fill in this section: The patient’s surname is written first, followed by the patient’s first name. If the patient has a middle name, write that in the space as well. Example: The patient’s name is Francis Mulenga
Sex • How to fill in this section: Circle the appropriate box for either male (M) or female (F) • Example: Francis Mulenga is male, “M”should be recorded
Age (in years) • How to fill in this section: The correct response for this column is age in years. If the patient is a child under one year old, write the number of months followed by /12. E.G., 6 months would be 6/12. • If the patient doesn’t know their age • Look on the OPD • Ask year of birth • Ask a family member
Omang/Passport # • How to fill in this section: Fill in the 9-digitOmang number or Passport number of each TB patient in the space provided. If the patient does not have an identification number, leave this column blank. • Example: Francis Mulenga’s Omang number is 123456789
Address in Full • How to fill in this section: The best description of where the patient lives should be written in this section (street address or plot number). The HCW needs to know enough to FIND the person if s/he has to!! • Example: Francis Mulenga lives in a blue house near the Shell petrol station in plot 45 • Request at least one mobile phone number for patient and close relative.
Registration and Transfer Information • How to fill in this section: • Unit TB No: The Unit TB number consists of four parts : • A: District Number • B: Health facility Code number • C: Specific serial number of the patient starting with 001 at the beginning of each year • D: Year of registration
Registration Number (2) • The first two parts of the number ('A' and 'B') are common to all patients registered in one health facility. The parts 'C' and 'D' are specific to each patient • Example: A patient (NOT Francis Mulenga) was registered in District 15 (‘A’ = 15), in Bontleng Clinic ('B’ = 302), and is the 89th registered patient ('C' = 89) in the year 2004 ('D' = 04) 302
Registration Number (3) • Block “C” IDs should begin at 001 on January 1st of each year and proceed sequentially. • Each patient is given a unique ID each time s/he is registered • Patients returning after default or failure should be RE-registered with a new unique ID • If a mistake is detected, never renumber all the patients and do not use white out. EVER. • a patient is registered twice for same treatment episode, • TB is “ruled out” • a numbering error occurred (duplicates or skips) 302
Registration Number (3) • In the event a numbering error occurred, draw a line through the entry and re-enter at the end of the list of patients • This pertains to duplicate entries of the same patient with different numbers or duplicate entries of same number different patient • Make a note in remarks which explains why the patient is registered out of sequence • Do not re-assign a registration number once used • NO TIPEX!!
Transfer information (3) Transferred/Moved Out: • If a patient transfers to a facility in another district during treatment (“transfer out”), or moves to another facility in the same reporting unit (“move out”), fill in the “To” column with the name of the health facility to which the patient transferred /moved. • The BNTP form entitled Notice of Transfer of a Patientmust be completed for all patients transferring or moving • The form should be sent with the patient • A duplicate Omang TB treatment card should be sent with the patient to the new facility • The original form should remain at originating clinic
Transfer information (4) • Example: a patient with registration number “089/04” was moved out to Ext. 14 Clinic on 02 October 2004.
Transfer information (5) Transferred/Moved In: • Patients transferred or moved in from another reporting unit to your health facility, should be (re) registered in the TB register. Enter your unit TB number, along with the patient’s new registration number, in the second line of the box. Put an “X” in the “IN” column • Note that this is a duplicate TB treatment card, as the original card remains at the original health facility • The receiving clinic must complete the Response to aTransfer of a Patientand return to sending clinic.
Transfer information (6) • Do not fill in the “REGISTERED” column. This column simply states that the patient has been registered in your health facility. Record the date that the patient came into health facility • Example: the patient was re-registered with the new registration number “078/04”, when he moved in to Ext. 14 Clinic on 15 October 2004
TB Classification (1) • Purpose: Disease classification and site of disease should be recorded in this section. • Pulmonary disease means TB of the lungs, including patients that are smear-positive or smear-negative. • All other types of TB are classified as extrapulmonary disease, including pleurisy and miliary TB • Patients with pulmonary AND extrapulmonary disease should be classified as pulmonary
TB Classification (2) • How to fill in this section: Make an “X” over the appropriate box for pulmonary TB or extrapulmonary TB • If the patient has both pulmonary and extrapulmonary TB, mark this as pulmonary TB and fill in the site of extrapulmonary TB. • In the case of extrapulmonary TB, indicate the site that has been affected in the space provided • Example: Francis Mulenga has pulmonary TB
Patient Category • The proper category of patient is necessary to determine the appropriate treatment regimen. • How to fill in this section:Make an “X” over the box with the appropriate option. The four options are: • NEW • FAILURE • DEFAULT • RELAPSE • Francis Mulenga is a new patient RETREATMENT CASES
Sputum Examination Results – Pre-treatment (1) • Purpose: These columns record the date and results of the patient’s pre-treatment sputum smear result. In all cases (except young children), three sputum examinations should be done (spot, morning, spot) • How to fill in this section: Using the format “dd/mm/yy”, fill in the sputum collection date. • The correct responses for the Results column are “P” for positive and “N” for negative. Indicate the grading of the sputum result (i.e. scanty, +, ++, +++)
Sputum Examination Results – Pre-treatment (2) • Example: Francis Mulenga gave three sputum specimens for examination, one on 12th January and two on 13th January. The results were “+++”, “++”, and “+++”, respectively
Intensive phase (2 month exam) • Purpose: Two sputum smears should be done after two months of treatment. • How to fill in this section: Using the format “dd/mm/yy”, fill in the date of collection of sputum. The correct responses for the Results column are “P” for positive and “N” for negative. Indicate the grading of the sputum result (i.e. scanty, +, ++, +++) • Example: Francis Mulenga gave one sputum specimen for examination on 15th March. The result was negative.
Sputum Smear Results – End of Treatment (6 months) • Two sputum examinations should be done at the end of six months of treatment. • One negative smear is sufficient at the end of Category I treatment • How to fill in this section: Using the format “dd/mm/yy”, fill the date of collection of sputum. • Example: Francis Mulenga gave two sputum specimens for examination on 5th July. The results were negative • No patient is considered CURED without a recorded, negative 6- month sputum exam result!!
Sputum Smear Results – End of Treatment (8 months) • Category II patients should have two sputum examinations at 8 months. • How to fill in this section: Using the format “dd/mm/yy”, fill in the Date column with the date of collection of sputum. The correct responses for the Results column are “P” for positive and “N” for negative. Indicate the grading of the sputum result (i.e. scanty, +, ++, +++)
Pre-treatment Weight • This section records the patient’s weight prior to treatment, in kilograms • How to fill in this section: Weigh the patient and record the value in the space provided • Weight is essential to determine drug dosages
Initial Phase of Treatment • This section lists the fixed-dose combinations of anti-TB drugs for adults and children during the intensive phase of TB treatment • How to fill in this section: Circle the anti-TB regimen that the patient is taking • Example, Francis Mulenga weighs 58 kg, so he will receive the regimen circled
HIV Status • This section records up to two HIV test results for each TB patient. • Patients with a negative test result at the beginning of treatment should be re-tested within three months or before the end of treatment • Example: Francis Mulenga was tested HIV negative on 15 January 2005; make an “X” over the box indicating a negative result and record the date • Francis Mulenga was retested two months later and had a positive test result; make an “X” over the box indicating a positive result and record the date X X 15/03/05
ART: Antiretroviral Therapy • This section records TB patient history of, or concurrent treatment with ART, along with the date • How to fill in this section: Make an “X” over the appropriate box. If the patient is on ART, or has a history of taking ART, make an “X” in the “Yes” box. If the patient is HIV negative, leave the box blank. If the patient is HIV-infected, but is not on ART, mark the box “NO”. Using the format “dd/mm/yy”, record the date in the appropriate column • Example: The patient is not currently on ART; make an “X” over the “No” box on the treatment card X
IPT-Isoniazid Preventive Therapy • This section records whether the TB patient has received isoniazid preventive therapy (IPT) prior to the current TB episode, along with the date IPT started • How to fill in this section: Make an “X” over the appropriate box. If the patient has ever taken even one dose of IPT as part of the IPT programme , make an “X” in the “Yes” box. If the patient has never taken IPT, make an “X” in the “No” box. Using the format “dd/mm/yy”, record the date in the appropriate column • Example: The patient received 3 months of IPT prior to developing TB; mark an “X” over the “YES” box on the treatment card X 15/03/05 X 01/06/03
Other tests – Biopsy • This section records biopsy results for each TB patient, along with the date. Not all TB patients will have a biopsy, so this section may be left blank if it is not applicable • How to fill in this section: Using the format “dd/mm/yy”, record the date in the appropriate column. The correct responses for the Results column are “P” for positive and “N” for negative
Other tests – PPD • How to fill in this section: Using the format “dd/mm/yy”, record the date in the appropriate column. The correct response for the Results column is the number of millimeters (mm) of the test result • Example: Francis Mulenga had a PPD result of 18 millimeters on 15 January 2005. The section would be completed as shown
Other tests – Other • How to fill in this section: Using the format “dd/mm/yy”, record the date in the appropriate column. The correct response for the Results column will vary depending on the type of test • Example: Francis Mulenga did not have any other tests performed, so this section will be left blank
Treatment Compliance • This section can be used to track patient adherence to anti-TB treatment on a daily basis. It also records the follow-up weight at the end of each calendar month • How to fill in this section: HCW should enter his/her initials on each day of supervised drug administration, a “-“ for self-supervised treatment, or a “0” for any missed treatment • Example: Francis Mulenga began DOT on 15 January, 2005. On 22 January, he was unable to visit the clinic and missed that day of treatment. His follow-up weight at the end of January was 59.2 kilograms
Continuation Phase of Treatment • This section lists the fixed-dose combinations of anti-TB drugs for adults and children during the continuation phase of treatment • How to fill in this section: Record the patient’s follow-up weight and circle the anti-TB regimen that the patient is taking • Example: Francis Mulenga weighs 59.4 kg at the continuation phase of treatment, so he will receive the regimen circled
Contact Screening • This section records the number of people that the TB patient thinks s/he has come in contact with, along with the number of contacts screened for TB using • How to fill in this section: Record the number of people that the TB patient thinks they have come in contact with in the first column. Of these people, record the number of contacts screened for TB using the BNTP screening form. • Example: Francis Mulenga thinks he came in contact with 5 people. Of these, 3 people have been screened for TB
Chest X-Ray • Record results for up to two chest x-rays, along with the date of the chest x-ray • How to fill in this section: Record the chest x-ray number in the first section. Draw any abnormalities in the corresponding location on the picture of the lungs. Using the format “dd/mm/yy,” record the date in the appropriate column • Example: A patient has a cavity in the right upper lobe, according to his chest x-ray from 25 December, 2004, x-ray number 2234. This section would be completed as shown above
Culture and Sensitivity Report • All re-treatment cases should submit a sputum specimen for culture and drug sensitivity testing. • If a culture was performed, this section can be used to record the results of the drug sensitivity profile for each TB patient, along with the date • How to fill in this section: Using the format “dd/mm/yy”, record the date in the appropriate column. If the sample is sensitive to a drug, mark the “Sensitive” column with an “X.” If the patient is resistant to a drug, mark the “Resistant” column with an “X” • Example: A culture was performed for a patient on 30 March, 2005. Her result showed sensitivity to all first-line drugs
Treatment Outcome • Categorise the outcome of each TB patient at the end of treatment • How to fill in this section: Fill in the column with the appropriate outcome: • Cured • Treatment completed • Treatment failure • Died • Defaulted/interrupted • Transferred out • Example: Francis Mulenga was initially smear-positive, but converted to smear-negative after two months of treatment. He had a smear-negative sputum result at 6 months. Therefore he is considered cured; make an “X” over the box for cured
Remarks • This section records specific information not captured by any of the other sections about each TB patient • How to fill in this section: Following are examples of what can be written in this section: • “Patient’s wife is HIV positive” • “CD4 count =50 on 12/03/05” • Example: Francis Mulenga’s wife is HIV-infected; record this information in the remarks section. This remark should also be a reminder that Francis should be offered another HIV test during his treatment
SECTION B: The TB Register • Backbone of the National TB Programme surveillance system • Information is recorded upon diagnosis and updated at each follow-up visit
Completing the TB Register The example register is taken from Bontleng Clinic.
Registration Number • The registration number provides each TB patient with a unique identification number. Patients should be assigned a registration number upon TB diagnosis • How to fill in this column: The registration number consists of the consecutive patient number (starting at “1” at the beginning of each calendar year) and the year of registration • Example, Francis Mulenga is the first patient in the register for 2005. Therefore, his registration number will be “001/05”