Download
1 / 1
10 likes | 85 Vues
Investigating how executive functioning difficulties impact social, emotional, and behavioral challenges in children with NF, exploring correlations between behavior regulation and adaptive functioning. Findings suggest executive dysfunction predicts externalizing and internalizing symptoms, influencing daily functioning at home and school.

E N D
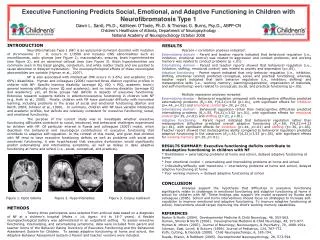
INTRODUCTION Neurofibromatosis Type-1 (NF) is an autosomal dominant disorder with mutation of chromosome 17. It occurs in 1/3500 and includes CNS abnormalities such as neurofibromas, optic gliomas (see Figure 1), macrocephaly, seizures, brain hyperintensities (see Figure 2), and an abnormal callosal area (see Figure 3). Brain hyperintensities are commonly seen in the basal ganglia, cerebellum, and white matter tracts and are posited to cause abnormal or delayed myelination. The neuropsychological effects of these neurological abnormalities are variable (Hyman et al., 2007). NF is also associated with intellectual (MR occurs in 3-6%) and academic (30-69%) disabilities. Hyman and colleagues (2006) reported three distinct cognitive profiles in children with NF: Specific learning disability (average IQ, VIQ < PIQ, academic lower); general learning difficulty (lower IQ and academic); and no learning disability (average IQ and academic); yet, all three groups had deficits in aspects of executive functioning. Extensive research supports deficits in attention/executive functioning in children with NF (e.g. Koth et al., 2000). Finally, children with NF have particular difficulty with nonverbal learning, including problems in the areas of social and emotional functioning (Barton and North, 2004; Johnson et al., 1999). In summary, children with NF have variable intellectual and academic profiles, but deficits are relatively consistent for executive functioning, social, and emotional functioning. The purpose of the current study was to investigate whether executive functioning difficulties contribute to social, emotional, and behavioral challenges experienced by children with NF. Of particular interest is Rueda and colleagues (2005) model, which describes the behavioral and neurological contributions of executive functioning that contribute to adaptive self-regulation. In the context of this model, and given that children with NF tend to have executive functioning deficits as well as problems with social and emotional functioning, it was hypothesized that executive dysfunction would significantly predict externalizing and internalizing symptoms, as well as delays in daily adaptive functioning at home and school (i.e., social, conceptual, and practical). Figure 1. Optic Glioma Figure 2. Hyperintensities Figure 3. Corpus Callosum METHODS Twenty-three participants were selected from archival data based on a diagnosis of NF at a children’s hospital (Males = 14; Ages= 4-4 to 18-7 years). A flexible neuropsychological battery was administered in an outpatient setting. To assess executive functioning, internalizing, and externalizing symptoms, data were included from parent and teacher forms of the Behavior Rating Inventory of Executive Functioning and the Behavioral Assessment System for Children. To assess adaptive functioning at home and school, the Adaptive Behavior Assessment System-2 Parent and teacher versions were included. RESULTS Pearson-r correlation analyses indicated: Externalizing domain - Parent and teacher reports indicated that behavioral regulation (i.e., inhibition, emotional control) was related to aggression and conduct problems; and working memory was related to conduct problems (p <.01). Internalizing domain - Parent and teacher reports showed that behavioral regulation (i.e., inhibition, shifting, emotional control) was related to anxiety and depression (p<.05). Adaptive functioning - Parent report indicated that only behavior regulation (i.e., inhibition, shifting, emotional control) predicted conceptual, social, and practical functioning; whereas, teacher report indicated that both behavior regulation (i.e., inhibition, shifting) and metacognitive skills (i.e., working memory; planning/organization, organization of materials, and self-monitoring) were related to conceptual, social, and practical functioning (p<.05). Multiple regression analyses revealed: Externalizing domain - Behavioral regulation compared with metacognitive difficulties predicted externalizing problems (R2=.69, F(4,21)=4.54 (p<.01), with significant effects forinhibition (b=.44, p<.01) andemotional control(b=.30, p<.01). Internalizing domain - Behavioral regulation rather than metacognitive difficulties predictedinternalizing problems (R2=.55, F(4,21)=3.52 (p<.01), with significant effects foremotional control(b=.35, p<.01) andshifting(b=.21, p<.01). Adaptive functioning - Parent report indicated that behavioral regulation rather than metacognitive difficulties predicted overall adaptive functioning (R2=.60, F(4,21)=4.23 (p<.01), with significant effects forinhibition(b=.44, p<.01) andshifting (b=.30, p<.05). Teacher report showed that metacognitive ability compared to behavioral regulation predicted adaptive functioning in the classroom (R2=.43, F(4,21)=3.53 (p<.05), with significant effectsforworking memory(b=.20, p=.01). RESULTS SUMMARY: Executive functioning deficits contribute to maladaptive functioning in children with NF * Disinhibition = externalizing problems at home and school, delayed adaptive functioning at home * Poor emotional control = externalizing and internalizing problems at home and school * Inflexibility/difficulty with transitions = internalizing problems at home and school, delayed adaptive functioning at home * Poor working memory = delayed adaptive functioning at school CONCLUSION Analyses support the hypothesis that difficulties in executive functioning significantly relate to challenges in emotional functioning and adaptive functioning at home in school for children with NF. These findings also support the model proposed by Rueda and colleagues (2005). School and home interventions should focus on strategies to increase self-regulation to improve emotional and adaptive functioning. To improve adaptive functioning at school, interventions should target improving the child’s working memory capabilities. REFERENCES Barton & North (2004). Developmental Medicine & Child Neurology, 46, 553-563. Hyman, Shores & North (2006). Developmental Medicine & Child Neurology, 48, 973-977. Hyman & others (2007). Journal of Neurology, Neurosurgery, & Psychiatry, 78, 1088-1091. Johnson, Saal, Lovell, & Schorry (1999). Journal of Pediatrics, 134, 767-772. Koth, Cutting, & Denckla (2000). Child Neuropsychology, 6, 185-194. Rueda, Posner, & Rothbart (2005). Developmental Neuropsychology, 28, 573-594. Executive Functioning Predicts Social, Emotional, and Adaptive Functioning in Children with Neurofibromatosis Type 1Dawn L. Ilardi, Ph.D., Kathleen O’Toole, Ph.D. & Thomas G. Burns, Psy.D., ABPP-CNChildren’s Healthcare of Atlanta, Department of NeuropsychologyNational Academy of Neuropsychology October 2008





