Immunologic Tolerance
Immunologic Tolerance. Contents. Part Ⅰ Introduction Part Ⅱ Development of Immunologic Tolerance Part Ⅲ Mechanism of Immunologic Tolerance Part Ⅳ Immunologic Tolerance and Clinic Medicine. Part Ⅰ Introduction.

Immunologic Tolerance
E N D
Presentation Transcript
Contents • Part Ⅰ Introduction • Part Ⅱ Development of Immunologic Tolerance • Part Ⅲ Mechanism of Immunologic Tolerance • Part Ⅳ Immunologic Tolerance and Clinic Medicine
Part Ⅰ Introduction • Definition:A type of specific unresponsiveness to an antigen induced by the exposure of specific lymphocytes to that antigen, but response to other antigens normally. • Tolerogens:antigens that induce tolerance
General features of Immunologic tolerance • Tolerance is antigenic specific and results from the recognition of antigens by specific lymphocytes. • Normal individuals are tolerant of their own antigens(self antigen)----- Self-tolerance. • Foreign antigens may be administered in ways that preferentially inhibit immune response by inducing tolerance in specific lymphocytes---antigen induction.
Immunologic features of tolerance • It is an antigen-induced, active process • Like immunologic memory, it is antigen specific • Like immunologic memory, it can exist in B cells, T cells or both • Like immunologic memory, its easier to induce and lasts longer in T cells than in B cell
Difference of Immuologic tolerance & immunodeficiency, immunosuppression Immunodeficiency: any condition in which there is deficiency in the production of humoral and /or cell-mediated immunity---non-specificity to Ag Immunosuppression: The suppression of immune responses to antigens. This can be achieved by various means, including physical, chemical----non-specificity to Ag
1. Induction of immunologic tolerance to antigen in fetal period and neonate period • Owen first observed immunologic tolerance to allogenic antigen in fetal period in 1945
2. Induction of immunologic tolerance to antigen in adult Antigen and immunologic tolerance: • Concentration of antigens • Type of antigen: monomer, aggregates • Pathway of antigen entering body • Features of determinant: tolerogenic epitope • Variation of antigen
Individual and immunologic tolerance: Heredity,Age, Gender, Health
Host age and antigen dose affect tolerance newborn adult
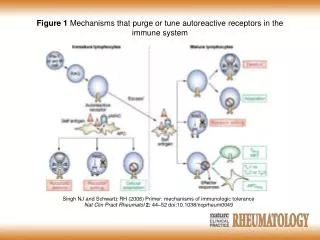
1. Central tolerance: Central tolerance occurs in the central lymphoid organs as a consequence of immature self-reactive lymphocytes recognizing ubiquitous self-antigen. 2. Peripheral tolerance: tolerance was induced in peripheral organs as a result of mature self-reactive lymphocytes encountering tissue-specific self antigens under particular conditions
1. Central tolerance Clonal deletion (apoptotic cell death) During maturation of lymphocytes in the thymus for T cell or in the bone marrow for B maturation, immature lymphocytes that recognize ubiquitous self-antigen with high affinity are deleted bynegative selection
2. Peripheral tolerance ① clonal deletion and clonal ignorance: large tissue specific antigen delete specific T cells. self-reactive lymphocytes remain viable and functional but do not react to the self antigens in any detectable way. ② Clonal anergy and inactivation: functional inactivation without cell death: lack co-stimulatory signal
③ Action of Suppressor lymphocyte (Ts) ④ Action of cytokines: TGF- , IL-10 ⑤ Holdbackin signal tranduction ⑥Immunologically privileged sites anatomic barrier: clonal ignorance
Pathways to Peripheral Tolerance Proliferation & differentiation Activated T cells NormalResponse B7 CD28 Antigen Recognitionwithout co-stimulation FunctionallyUnresponsive Anergy CTL4-B7 interaction CTLA4 B7 Fas Activation induced cell death Fas-FasL interaction Apoptosis FasL Inhibition of proliferation & effector action Cytokine-mediated suppression Cytokine regulation cytokines
TCR MHC II B7 CD28 The Two Signal Hypothesis for T-cell Activation Signal 1 Mature Dendritic cell APC Activated TH cell TH cell Signal 2
Resting B-cell APC TH0 cell CD28 Tolerance (anergy or apoptosis) from lack of signal 2 Hypothetical mechanism of tolerance in mature T cells Signal 1 Tolerant T cell
Proliferation & differentiation B7 CD28 Anergy Antigen Recognitionwithout co-stimulation Summary: Lack of co-stimulation can lead to tolerance (anergy) Activated T cells NormalResponse
CTLA4-B7 interaction FunctionallyUnresponsive (Anergic) T cell Regulation by CTLA-4 CTLA4 B7 Activated T cell
Regulatory T cells Production of IL-10 or TGF-b FunctionallyUnresponsive T cell RegulatoryT cell
Inhibition by Antibody Feedback • Passively administered antibody can prevent an antibody response • Antibody produced during an immune responses leads to elimination of antigen (stimulus) • Less antigen available to stimulate specific cells • Immune complexes can bind to inhibitory receptors Application: RhoGam for Erythroblastosis Fetalis
Major Immune Inhibitory Receptors • B cells • FcgRII • T cells • CTLA4 • NK cells • KIR (killer cell Ig-like receptors),
Anti-Idiotypes and Immune Regulation • Definition • anti-idiotype response-antibody produced against immunoglobulin or TCR idiotypes that serve to down-regulate immune response • The epitope for an responsive anti-idiotype molecule (antibody, BCR, or TCR) is the internal image formed by the CDR region of the respective epitopes antigen receptor
1. To induce immunologic tolerance • Prevent the rejection of organ allografts and xenografts • Treat autoimmune diseases • Treat allergic diseases
2. To terminate immunologic tolerance • To treat tumor: enhance first signal or second signal • To treat infection diseases
Patient Presentation • 6 year old male, ER with unexplained bruising associated with minor trauma • Patient has minimal clotting activity • FVIII levels <1% of normal • Patient given i.v. FVIII concentrate i.v. and released but returns in two weeks with same problem • Repeated FVIII treatment • However, FVIII is ineffective.
Issues • Coagulation factor inhibitors (anti-FVIII activity) • Basis? • Lack of tolerance. Why? • Prevalence/impact • 20-30% FVIII, less FIX • Treatment/problems • FVIII concentrate or rFVIII • Inhibitors develop that neutralize FVIII • Therapy? • Porcine FVIII with less cross-reactivity • Tolerance (high dose) • Gene therapy
What are Inhibitors? • IgG; commonly subclass 4, mixed 1 & 4 • Occur in • Congenital factor deficiency = alloimmune • Previously unaffected = autoimmune • Associated with pregnancy, autoimmunity, malignancy, multi-transfusion, advanced age etc.