Download
1 / 35
350 likes | 506 Vues
Measuring the burden of TB directly Surveys of TB infection and disease - Brian Williams (STB/TME) - Geneva Workshop June 2005. We want to reduce Morbidity and mortality New infections Recurrence of old infections Prevalent cases. Routine programme data. Notifications Cure rates

E N D
Measuring the burden of TB directly Surveys of TB infection and disease - Brian Williams (STB/TME) - Geneva Workshop June 2005
We want to reduce • Morbidity and mortality • New infections • Recurrence of old infections • Prevalent cases
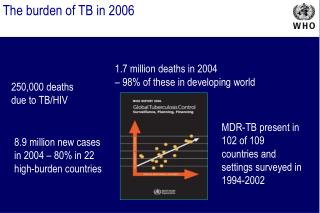
Routine programme data • Notifications • Cure rates • Drug resistance • Mortality • Process indicators
But... • Biases • Incompleteness • Recording • Reporting • Analysing • AIDS
Four things we can measure • Prevalence of infection (tuberculin surveys) • Incidence of infection (ARTI) • Incidence of disease • Prevalence of disease • Prevalence of HIV in TB patients
Measuring the prevalence of infection Tuberculin surveys
Sampling Districts: Probability proportional to size Schools in districts: Random Children in schools: Total sample within schools Sample size: Small to minimize costs and logistical problems; Large to get the most accurate estimate How many districts? How many schools in districts? How many children in schools?
Design effect Multiply your sample size by D. D = 1 + (m - 1)ρ where m is the number of people in each cluster and the intra-cluster correlation coefficient, ρ,is ρ = VB/VW with VBthe between-cluster variance and VWthe total variance. No difference between clusters: VB = 0, ρ = 0, D = 1. Members of a cluster are identical: VB= VW, ρ = 1, D = m
Tanzania 1983 to 1988 Egypt 1995 to 1997 15 10 5 0 4 2 0 Frequency (%) Frequency (%) BCG BCG No BCG No BCG 0 10 20 30 0 10 20 30 Size of induration (mm) Size of induration (mm) Korea
Calculating ARTI(R) from prevalence (P) and age (A) R = 1 – (1 – P)1/A Probability of being infected per year = R Probability of not being infected per year = 1 – R Probability of not being infected after A years = (1 – R)A 1 – P = (1 – R)A 1 – R = (1 – P)1/A
Assumptions The annual risk of infection is constant over time and independent of age. Surveys in school children, aged about 5 to 10 years: estimate of the ARTI is averaged over about five to ten years.
South Korea Halving in ln(2)/0.07 10 years 10 to 20 years 5 to 10 years
Calculating incidence from the ARTI Styblo showed that for every 1% increase in the annual risk of infection, the incidence of SS+ disease increases by (5010)/100,000/yr. If we multiply the ARTI by 50 this gives us an estimate of the incidence of SS+ TB.
Estimating sample sizes quickly If you count N positives then: N 95% confidence limits 2N Fractional error 2N/N = 2/N Incidence (South Korea, 1990) 40 per 100,000 95% confidence limits 2N = 13 ( 32%) Sample of 800,000 gives 320 positive 11%
South Korea Incidence Survey 1998: Baseline 920,000 had chest radiography 840,000 did not have suspicious CXR 1990: Follow up 790,000 available for CXR 2,500 with suspicious X-rays 2000 had sputa taken 200 smear positive 300 culture positive (smear negative)
South Korea ARTI50 Civil servants Rate of decline = 7.9%/yr
Measuring the prevalence of disease Same sampling problems as for incidence….
South Korea Rate of decline = 8.0%/yr
Incidence and prevalence It is easier to reduce prevalence than incidence. Duration of disease Prevalence/Incidence
Incidence and prevalence in South Korea Prevalence/100k Incidence/100k/yr Duration of disease/years Age/years
Smear positive disease in South African gold miners Incidence (%/yr) Prevalence (%) Dis.Duration (yr) HIV- 0.48 0.55 1.15 HIV+ 2.87 0.44 0.15 Ratio 6.01 0.80 0.13 Corbett et al. 2003
Changes in the annual risk of TB infection in Kenya (percent per annum) Early HIV Late HIV 1986-1990 3.7 5.9 1994-1996 11.3 6.9 Ratio 3.2 1.2 Early HIV: Kisii, South Nyanza, Kakamega, Siaya, Nairobi Late HIV: Nakuru, Muranga, Kitui, Elgeyo Marakwet, Meru Odhiambo et al. Am. J. Pub. Health (1999)
Changes in the annual risk of TB infection in Tanzania (percent per annum) 1995 1.10 2000 0.67 Ratio 0.61 Egwaga et al. TSRU meeting, Bagamoyo India
The incidence of SS+ tuberculosis plotted against the prevalence of HIV for African countries in 2001.
Williams, B. G. & Dye, C. Antiretroviral Drugs for Tuberculosis Control in the Era of HIV/AIDS Science (2003) 301 1535-1537.
Reduction in the life-time incidence of TB among HIV positive people Williams, B. G. & Dye, C. Antiretroviral Drugs for Tuberculosis Control in the Era of HIV/AIDS Science (2003) 301 1535-1537.
We think that DOTS should continue to work for HIV-negative people and HIV-positive people need ART. But how do we stop transmission?