OUR TECHNIQUE FOR THE HYBRID PROCEDURE IN HYPOPLASTIC LEFT HEART SYNDROME
OUR TECHNIQUE FOR THE HYBRID PROCEDURE IN HYPOPLASTIC LEFT HEART SYNDROME. Drs. Luis León, Stephan Haecker, Daniel Pérez, Luis Cárdenas, Miguel A. Santis. Centro Cardiovascular Pediátrico, Clínica Santa María, Santiago,Chile.

OUR TECHNIQUE FOR THE HYBRID PROCEDURE IN HYPOPLASTIC LEFT HEART SYNDROME
E N D
Presentation Transcript
OUR TECHNIQUE FOR THE HYBRID PROCEDURE IN HYPOPLASTIC LEFT HEART SYNDROME Drs. Luis León, Stephan Haecker, Daniel Pérez, Luis Cárdenas, Miguel A. Santis. Centro Cardiovascular Pediátrico, Clínica Santa María, Santiago,Chile.
*The Norwood procedure is our first choice in the surgical treatment of Hypoplastic Left Heart Syndrome. *We have adopted the HYBRID PROCEDURE as an emergency treatment whenever the Norwood operation carries a higher risk due either to poor preoperative hemodynamic conditions, or to severe pediatric problems. *The Hybrid Procedure may offer inmediate hemodynamic gain and an improved outcome in these patiens.
HYBRID PROCEDURE TECHNIQUE STAGE 1 IN THE PEDIATRIC CARDIAC OPERATING ROOM BANDING RIGHT AND LEFT PULMONARY ARTERY
STAGE 1 1. STERNOTOMY 2. PREPARING GORETEX BANDS 3. RPA AND LPA DISSECTION 4. RPA BANDING 5. LPA BANDING AORTA ductus RPA LPA PA LV RV
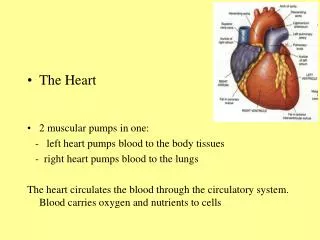
*STERNOTOMY *FINDINGS: dilated PA at systemic presure, minute aorta(2,5-3,5 mm), very large patent ductus obscuring the LPA Ductus aorta Pulmonary artery Right Ventricle
*Limited dissection between PA and aorta reduces the chance of inadvertent occlusion Ductus aorta Pulmonary artery Right Ventricle
*Two Goretex rings 2 to 3 mm wide are produced from a 3.5 mm tube Goretex 3.5 mm 3.5 GORETEX TUBE
*A 5/0 Prolene mattress stitch is sutured on the upper end keeping near the free edge *After surrounding the PA branch the suture is passed through the lower end and tied
*RPA & LPA banding does not require pump support
*The assistant surgeon carefully displaces the pulmonary artery and aorta towards the left, avoiding both aortic occlusion (myocardial ischemia) and ductal occlusion (sistemic hypotension), as well as pulmonary valve distortion (sistemic valve incompetence) *a traction suture is placed on the right atrial appendage if necessary RPA SVC RA
*a minimum of dissection around the RPA is necessary *the Goretex ring is passed behind it, and the artery is subsequently banded
*the Goretex ring is passed behind it, and the artery is subsequently banded
*the right pulmonary artery is now banded.
The assistant surgeon will now displace both arteries to the right, revealing the LPA. Again, kinking the aorta, occluding the PDA and producing pulmonary valve incompetence are carefully avoided. LPA
Limited dissection around the LPA origin Is necessary.
The second Goretex ring is passed behind the LPA and sutured The external diameter of the banded LPA is approximately 3 mm
The second Goretex ring is passed behind the LPA and sutured The external diameter is approximately 3 mm
The external diameter is approximately 3 mm. It can be further reduced with an additional stitch • HEMODYNAMIC CHANGES: • Systolic and diastolic pressure increase, and so does systemic flow. • Pulmonary flow is moderately reduced, expected PO2 is 40 to 50 mm Hg • with O2 sat ranging from 80 to 90%
HYBRID PROCEDURE TECHNIQUE STAGE 2 IN THE PEDIATRIC CATH LAB PATENT DUCTUS STENTING
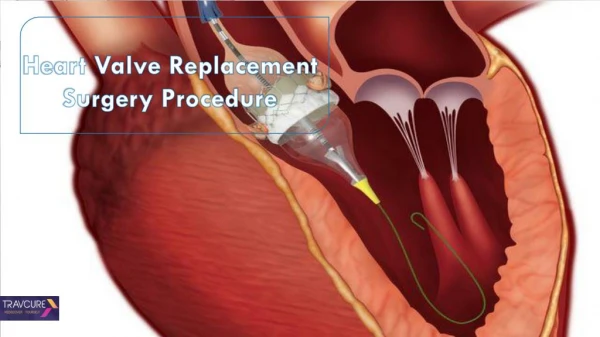
STAGE 2 Sternotomy A pursestring suture is placed in the sinotubular junction of the pulmonary artery. 2. A catheter intoducer is advanced 3. PA angiogram 6. Ductus measurements and STENT CHOICE 7. DUCTAL STENT DELIVERY
a Prolene pursestring • is placed at the sinotubular junction of the pulmonary artery
*A Nº7 intoducer is advanced into the PA *it is positioned 5 mm inside the PA *a test injection is performed
* ANGIO INFORMATION: * Ductus shape *Aortic arch shape (it may superimpose on the PDA) *Degree of branch PA banding
DUCTUS MEASUREMENT ductus width is measured at the pulmonary end
DUCTUS MEASUREMENT *Duct length is now measured along its center
STENT CHOICE *THE DUCT STENT MUST BE 1 OR 2 MILIMETERS LARGER THAN THE DUCT WIDTH (Eg: 8 mm stent for a 7 mm Duct ) *SELF EXPANDING DUCT STENTS ARE USUALLY 20 MM LONG *Baloon dilatation of a normal stent will stop systemic flow during the procedure 8 mm 20 mm
COLOCACIÓN DEL STENT *Stent Delivery: *The guide wire is advanced across the duct far into the descending aorta
COLOCACIÓN DEL STENT *The stent device is now in place: *The sheath has two radioopaque marks indicating de stent’s position
COLOCACIÓN DEL STENT *Stent delivery has begun as the cardiologist removes the sheath and a second cardiologist ,or surgeon holds the introducer during radioscopy *The stent tips are radioopaque. They show the actual position of the stent. Minor changes in position can still be achieved. If the stent has moved inwards, gently pull the introducer back.
COLOCACIÓN DEL STENT *The stent is 50% delivered. The position looks right
COLOCACIÓN DEL STENT *The stent is fully expanded *It is important that the proximal end be stented
COLOCACIÓN DEL STENT *We perform a final injection to check on flow through the ductus and retrograde flow in the aortic arch.
ç CASE 2 *Chest X-ray: The stent is shown in the anteroposterior view
CASE 2 *stent in lateral view
CASE 1 Angiogram for ductus measurement and stent choice
CASE 1 Ductal stent being delivered
CASE 1 Angiogram showing ductal and aortic patency after stent delivery
CASE 2 Angiogram for ductus measurement and stent choice
CASE 2 Angiogram evaluation of branch PA banding
CASE 2 Angiogram for ductus measurement and stent choice Inyección para medición del ductus y elección del stent
CASE 2 Ductal stent being delivered, initial phase Colocación del stent ductal
CASE 2 Ductal stent delivery completed Colocación del stent ductal
CASE 2 Angiogram showing ductal and aortic patency after stent delivery
CASE 3 Angiogram for ductus measurement and stent choice
CASE 3 Ductal stent being delivered
CASE 3 Angiogram shows that the proximal end of the duct is not covered by the stent
CASE 3 Second ductal stent being delivered
CASE 3 Angiogram showing ductal and aortic patency after second stent