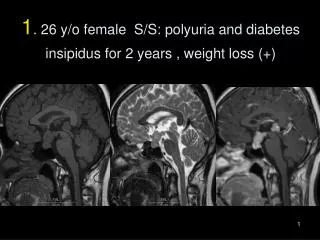
Download
1 / 56
2.29k likes | 6.13k Vues
Diabetes Insipidus. Endocrinology Rounds November 4, 2009 Selina Liu PGY4 Endocrinology. Objectives. To understand and describe the pathophysiology of diabetes insipidus To be able to diagnose and treat diabetes insipidus. Objectives. To name this statue, and its location

E N D
Diabetes Insipidus Endocrinology Rounds November 4, 2009 Selina Liu PGY4 Endocrinology
Objectives • To understand and describe the pathophysiology of diabetes insipidus • To be able to diagnose and treat diabetes insipidus
Objectives • To name this statue, and its location • EXTRA CREDIT: to learn when this statue was built
Outline • Background • Vasopressin Physiology • Definition & Classification of Diabetes Insipidus (DI) • Central Diabetes Insipidus • Causes & Pathophysiology • Approach to Polyuria & Diagnosis of DI • Treatment
Background - Vasopressin • Arginine Vasopressin (AVP) or Antidiuretic Hormone (ADH) • polypeptide hormone • synthesized in magnocellular neurons originating in hypothalamic nuclei - supraoptic and paraventricular • neurons terminate on capillaries of inferior hypophyseal artery of posterior pituitary • rapidly metabolized in liver & kidneys - t1/2 15-20 min Kronenberg HM et al. 2008 Williams Textbook of Endocrinology. 11th edition.
http://www.colorado.edu/intphys/Class/IPHY3430-200/image/figure1806.jpghttp://www.colorado.edu/intphys/Class/IPHY3430-200/image/figure1806.jpg
Background – Vasopressin Effects • mediated via GPCRs - vasopressin receptors V1, V2, V3 • V1 – vascular smooth muscle (liver, platelets, CNS) - increase peripheral vascular resistance - stimulate prostaglandin synthesis - stimulate liver glycogenolysis • V2 – renal - increase H2O permeability of the renal collecting duct epithelium via aquaporin-2 - stimulate vascular endothelial release of vWF, FVIII • V3 – pituitary - potentiate action of CRH ACTH release
Background – Vasopressin Effects • main effects: • regulation of water homeostasis and osmolality of body fluids • cardiovascular effects http://www.healthsystem.virginia.edu/internet/dab_lab/lecture_notes/pdf/adh.pdf
Background – Vasopressin Regulation Osmoregulation: • osmoreceptors in hypothalamus • sense increase in plasma osmolality • increase thirst and vasopressin secretion • increase fluid intake and water retention
Background – Vasopressin Regulation Osmoregulation: www.utdol.com
Background – Vasopressin Regulation Baroregulation: • baroreceptors in carotid sinus (also in left atrium – to lesser degree) • sense decrease in effective circulating volume by resultant decrease in cardiac output • less sensitive than osmoreceptors: - small changes in ECV – stimulate RAAS - only large changes in ECV – stimulate vasopressin secretion via baroreceptor
Background – Vasopressin Regulation Baroregulation: www.utdol.com
Background – Vasopressin Regulation • physiological & pathological factors affecting vasopressin secretion: www.utdol.com
3-4 pmol/L maximum urine concentration 0.5 pmol/L maximum diuresis Ball SG. 2007 Ann Clin Biochem 44:417-431
Diabetes Insipidus - Definition • insipidus – Latin (in + sapidus) – “tasteless” • characterized by large volume of hypotonic, dilute, tasteless urine • diabetes mellitus – hypertonic & sweet urine • polyuria – urine output >40ml/kg/day or >3L/day
Diabetes Insipidus: Classification • 4 pathophysiological mechanisms: • Primary Polydipsia (Dipsogenic DI vs. Psychogenic Polydipsia) • Nephrogenic Diabetes Insipidus • Transient Diabetes Insipidus of Pregnancy • Central Diabetes Insipidus (Hypothalamic or Neurohypophyseal DI)
Dipsogenic Diabetes Insipidus • abnormality in osmoregulation of thirst • ingestion of excessive volumes of fluid • suppression of vasopressin release polyuria • causes: • vs. psychogenic polydipsia – no abnormality in thirst? • idiopathic • infiltrative (sarcoidosis) • autoimmune (MS) • drug-induced (lithium, TCAs)
Nephrogenic Diabetes Insipidus • renal resistance to vasopressin • plasma vasopressin levels normal or elevated • causes: • chronic renal disease (any disorder interfering with collecting duct or medullary function i.e. PCKD, pyelonephritis) • familial/congenital – mutations in V2R, aquaporin-2 genes • drugs – lithium, demeclocycline, colchicine, gentamicin • hypercalcemia, hypokalemia • multiple myeloma, sickle cell anemia, Sjögren’s
Transient DI of Pregnancy Normal pregnancy: • reset osmostat plasma Na decreased by 5 mEq/L mediated by increase in hCG • increased catabolism of vasopressin due to cysteine aminopeptidase (vasopressinase) produced by placenta vasopressin levels usually remain normal due to increased production of vasopressin • water retention - fall in plasma osmolality 10 mOsm/kg • vasopressin release and osmotic threshold for thirst also decrease in parallel
Transient DI of Pregnancy • 2 types of DI in pregnancy • “vasopressin-resistant DI of pregnancy” • increased vasopressinase levels and activity • associated with pre-eclampsia, AFLP • accelerated catabolism of vasopressin in women with underlying borderline vasopressin function (i.e mild nephrogenic DI or partial central DI) • related to limited neurohypophyseal secretory reserve
Central Diabetes Insipidus • deficient vasopressin secretion • can cause variable degree of polyuria • defect at > 1 site involved in vasopressin secretion: • hypothalamic osmoreceptors • supraoptic or paraventricular nuclei • pituitary stalk
Makaryus AN & McFarlane SI 2006 Clev Clin J Med 73:(1)65-71
Central Diabetes Insipidus - Causes • Idiopathic • Familial • Trauma or Neurosurgery • Malignancy • Infiltrative • Hypoxic encephalopathy • Other
Idiopathic Central Diabetes Insipidus • destruction of hypothalamic secretory cells • ? autoimmune • cytoplasmic autoantibodies to vasopressin cells • lymphocytic infiltration of posterior pituitary & stalk • may also have anterior pituitary deficiency • possibly represents occult pathological process pts with idiopathic CDI who develop anterior pituitary deficiency years later may have pituitary or sellar tumour
Familial Central Diabetes Insipidus • autosomal dominant – mutation in AVP gene • accumulation of misfolded AVP precursors in ER • potentially toxic autophagy activated • results in apoptosis • progressive deficiency of vasopressin • signs & symptoms develop months to years after birth
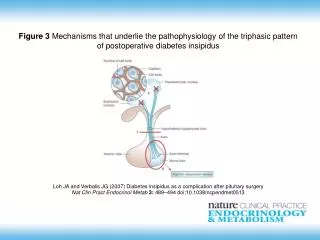
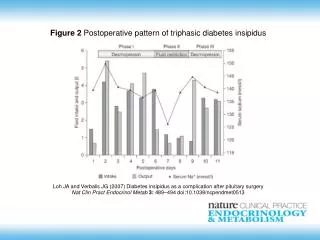
Post-Operative or Post-Trauma DI • transient DI within 24 hrs of pituitary surgery up to 50-60% of pts, usually resolves • if complete stalk section, can have triphasic response • initial polyuric phase – due to inhibition of vasopressin release due to hypothalamic dysfunction, - within first 24 h, lasts 4-5 d • antidiuretic phase – due to release of stored hormone - from day 6-12 • return of diabetes insipidus
Kronenberg HM et al. 2008 Williams Textbook of Endocrinology. 11th edition.
Post-Operative or Post-Trauma DI • estimated incidence post-pituitary surgery: • minimally invasive (endoscopic trans-nasal resection) • permanent 2.7%, transient 13.6% • elevated serum Na >145 within 5 days of surgery was predictive of developing permanent DI • sensitivity 87.5%, specificity 83.5%, NPV 99.5% • other risk factors: Rathke’s cleft cyst histology, intraoperative CSF leak, prev non-endoscopic resection Sigounas DG et al. 2008. Neurosurg 62:71-79
Other Causes of Central DI • Malignancy – both solid & hematological - 1o and metastatic • Infiltrative – Langerhans cell histiocytosis, sarcoidosis, autoimmune lymphocytic hypophysitis, Wegener’s • Hypoxic encephalopathy – cardiac arrest, shock, Sheehan’s syndrome • post-SVT correction – decreased AVP, increased ANP • anorexia nervosa • Acute Fatty Liver of Pregnancy
Wolfram’s Syndrome (DIDMOAD) • DIDMOAD – autosomal recessive • mutations in WFS1 (Wolframin) and ZCD2 genes encode endoplasmic reticulum proteins, involved in calcium homeostasis • Diabetes Insipidus – loss of AVP secreting neurons in supraoptic nuclei, impaired processing of AVP precursors • Diabetes Mellitus • Optic Atrophy • Deafness
Approach to Polyuria • History • onset/rate of polyuria, FMHx, medications • rule out other causes (osmotic diuresis, post-obstructive, diuretics, nocturia due to BPH etc.) • Physical Exam • fluid status assessment • Lab Investigations • serum & urine electrolytes, osmolality
Lab Test Central DI Nephrogenic DI Psychogenic Polydipsia Plasma osmolality Urine osmolality urine osm < plasma osm Lab Investigations
Water Deprivation Test • to confirm DI • to distinguish between central vs. nephrogenic • can be done as outpatient through CIU • under closely monitored conditions • medications that may interfere with results: • lithium, phenothiazines, cyclophosphamide, TCAs, phenytoin, carbamazepine, clonidine
Water Deprivation Test • check baseline weight, BP, serum & urine osm, lytes • NPO (timing depends on individual) • q 1 hrs: weight, BP, urine volume & osmolality • q 2 hrs: plasma lytes & osmolality
Water Deprivation Test • continue until 1 of the following occurs: • weight decreases by > 5% • urine osmolality increases < 30 mosmol/kg for 3 hrs • serum Na > 150 mmol/L • plasma osmolality > 300 mosmol/kg • significant decrease of BP • urine osmolality > 600 mosmol/kg
Water Deprivation Test • if any of these criteria met (except urine osmol >600) give DDAVP 10 mg intranasal • check urine & serum osmolality 1 h post-DDAVP
Water Deprivation Test - Interpretation • Complete Central DI • urine osmolality will be minimally concentrated despite dehydration • will have significant increase in urine osmolality in response to dDAVP (at least 50%, up to 200-400%) • undetectable vasopressin levels at end of dehydration • Complete Nephrogenic DI • also minimal urine concentration despite dehydration • LITTLE/NO response of urine osmolality to dDAVP • HIGH vasopressin levels at end of dehydration
Water Deprivation Test - Interpretation • Partial Central DI vs. Primary Polydipsia – can be difficult • both – urine will concentrate with dehydration • often above plasma osmolality • but does not approach 800-1000 mOsm/kg (normal) • after dDAVP – in Partial Central DI, may have further concentration of urine (at least 10%) but no further increase in Primary Polydipsia • some pts with partial central DI – may be hyperresponsive to submaximal rise in AVP with dehydration (?receptor upregulation), so may not have response to exogenous dDAVP
Nussey SS & Whitehead SA. Endocrinology An Integrated Approach 2001
Example – Water Deprivation Test ? Diagnosis
Treatment – Nephrogenic DI • maintain adequate water intake • dietary salt restriction, diuretics (thiazides), NSAIDS • (if partial sensitivity, can use desmopressin) GOAL – to maintain mild state of sodium depletion • reduce solute load on kidney • enhance proximal tubular reabsorption • minimize loss of water
Treatment – Transient DI of Pregnancy • Desmopressin – synthetic analogue of vasopressin not catabolized by vasopressinase • has 2-25% oxytocic activity of vasopressin so minimal stimulation of oxytocin receptors of uterus • safe for mother & fetus • close monitoring of fluid status during delivery • post-partum, plasma vasopressinase decreases • may resolve or become asymptomatic
Treatment – Central DI • GOAL – decrease thirst & polyuria to acceptable levels • decrease interference on lifestyle • avoid overtreatment (risk of hyponatremia) • only drink when thirsty • most people with intact thirst mechanisms will be able to maintain adequate water intake • caution in elderly, those with disrupted thirst mechanisms
Treatment – Central DI Medications: • Desmopressin (DDAVP) • nasal spray/solution, oral tablet/melt, sc injection • if partial central DI: • chlorpropamide • carbamezepine • clofibrate • thiazide/NSAID
Treatment – Central DI • desmopressin acetate - DDAVP • Spray – metered dose 10 mg nasal spray (10-40 mg daily) • Rhinyle – 0.1mg/ml nasal solution (0.05ml = 5mg) • Tablets - 0.1 or 0.2 mg tablets (max 1.2 mg daily) • Injection - 1-4 mg sc daily • Melts - 60, 120, 240 mg oral disintegrating tablets • titrate to symptoms – start at hs to control nocturia • monitor polyuria, timing of “breakthrough” • daily weights may be helpful
Treatment – Central DI • chlorpropamide – 250-500 mg daily • long-acting sulfonlyurea • promotes renal response to vasopressin • carbamazepine – 100-300 mg bid • anti-epileptic • enhance renal response to vasopressin • clofibrate – 500 mg q 6h • fibrate • increases vasopressin release • thiazide or NSAID