Download
1 / 33
420 likes | 778 Vues
TECHNOLOGY IN REHABILITATION Neuromodulation. Deep Brain Stimulation Overview . Elena Draznin, MD Medical Director , Swedish Rehabilitation Unit .

E N D
TECHNOLOGY IN REHABILITATION Neuromodulation Deep Brain Stimulation Overview Elena Draznin, MD Medical Director , Swedish Rehabilitation Unit.
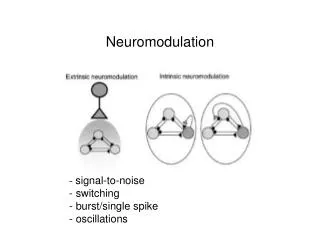
Neuromodulation is a therapeutic alteration of activity in central, peripheral or autonomic nervous systems, electrically or pharmacologically, by means of implanted devices Spasticity Parkinson’s disease, other movement disorders Cortical stimulation for stroke Pain Epilepsy Intractable nausea Cochlear implants
Idiopathic Parkinson’s disease • Progressive neurodegenerative disorder • 1.5 million in US • Slowly progressive • Asymmetric onset • Affecting mostly people over 60 • Etiology is unknown.
Two advocates for research who developed Parkinson's early: Muhammad Ali at age 42 and Michael J. Fox at age 30.
What Causes PD? A small area in the brain stem called the substantia nigra controls movement. In PD, cells in the substantia nigra stop producing dopamine, a chemical that helps nerve cells communicate. As dopamine-producing cells die, the brain does not receive the necessary messages about how and when to move.
Parkinson's Disease Brain disorder with a gradual loss of movement control. Cardinal signs : Tremors, Stiffness, rigidity Akinesia or bradykinesia. Postural instability, impaired balance.
Symptom: Tremor Tremor is an early symptom for about 70% of people with Parkinson's. It occurs in a finger or hand at rest, rhythmically, usually four to six beats per second, or in a "pill-rolling" manner, as if rolling a pill between the thumb and index finger.
TYPES OF TREMOR *Essential Tremor- 50% familial *Parkinsonism *Dystonia *Secondary tremor medicine stroke MS *Peripheral Nerve damage *Psychological
The early signs of Parkinson's disease include Stiffness or difficulty walking Difficulty getting out of a chair
The early signs of Parkinson's disease: Stooped posture A 'masked' face, frozen in a serious expression
Symptom: Rigidity Rigidity occurs when the muscles stay stiff and don't relax. The arms may not swing when a person is walking. There may be cramping or pain in the muscles.
Parkinson’s disease Cost of drug therapy $1,000- $6,000 per year Health care cost $2,000- $20,000 per year Risk of death doubles Referral to neurologist associated with decreased morbidity/ mortality and SNF placement.
Moderate to Advance Disease * On-off fluctuations random or EOD wearing off * Dose failures * Dyskenesias * Non dopamine responsive symptoms: postural flexion and instability falls retropulsion and propulsion freezing, motor initiation speech and swallowing
Mild Moderate Severe Disease Severity Dyskinesia, “On-Off” Motor Fluctuations Signs of levodopa“wearing-off” Postural Instability, Freezing, Falls, Dementia Patient Symptoms DBS Treatment Levodopa, COMT inhibitors, others Agonists Parkinson’s Disease Treatment: Continuum of Interventions Modified from Giroux, ML and Farris, SF. Cleveland Clinic Foundation 2005 Cleveland Clinic Foundation Center for Neurological Restoration
When Should DBS be Considered? • When, despite optimized pharmacotherapy, your patient experiences troubling motor symptoms, which may include: • Wearing off – Off periods that contain troubling bradykinesia, rigidity, tremor, and/or gait difficulty • Troubling dyskinesia • Motor fluctuations • Refractory tremor
Optimal candidate for DBS • Presence of on-off fluctuations • Dyskenesia impairing quality of life • Medication resistant tremor • Reasonable cognitive function • Adequate response to dopaminergic therapy
DBS: When Pharmacotherapy isn’t Enough • As Parkinson’s disease progresses, medications may fail to provide consistent and adequate symptom control • Medications used at levels required for symptom control may produce adverse effects • Motor complications, such as dyskinesia • Cognitive and psychiatric problems • Nausea, hypotension, and other systemic effects
Approved Indications • DBS Therapy is approved for the treatment of symptoms due to: • Essential Tremor • FDA approved in 1997 • Parkinson’s disease • FDA approved in 2002 • Dystonia • FDA approved (HDE*) in 2003 • Over 100,000 patients implanted worldwide *Humanitarian Device: Authorized by Federal Law for the use as an aid in the management of chronic, intractable (drug refractory) primary dystonia, including generalized and segmental dystonia, hemidystonia, and cervical dystonia, for individuals 7 years of age and older.
Team Screening for DBS • Neurologist • Neurosurgeon • Neuropsychologist • Physiatrist • Cost DBS $28,000 -- $50,000 • Programming cost $3,000
Dopamine dysregulation syndrome • Impulse control disorder: gambling, shopping, hypersexuality, • Behavior disturbances: aggressive tendencies, fights, psychosis, compulsive eating • Punding: repetition of complex motor behaviors • Hypomania, mania, dysphoria
Surgery: Deep Brain Stimulation Uses an implanted electrode to deliver high-frequency electrical stimulation to structures involved in the control of movement This electrical stimulation overrides abnormal neuronal activity within brain regions to bring motor controlling circuits into a more normal state of function, thereby reducing movement disorder symptoms
DBS Therapy • Acts on cells and fibers closest to the electrode, changing firing pattern of individual neurons in BG • Triggers neighboring astrocytes to release Ca2+ and neurotransmitters • Increases blood flow, stimulates neurogenesis Click screen to play
Target Sites for DBS Ventral Intermediate Thalamus: Essential Tremor Subthalamic Nucleus: Parkinson’s diseaseand Dystonia Globus Pallidus: Parkinson’s diseaseand Dystonia
DBS for Parkinson Disease GPi STN
Lesion therapy DBS • Thalamotomy • Subthalamotomy • Pallidotomy • High risk with bilateral lesion • Programmable • Bilateral placement • Reversible effect
DBS Therapy Steps • Inpatient admission for lead implant • Inpatient or outpatient admission for placement of implantable pulse generator. • Follow-up programming of IPG(s) • Rehabilitation
Inpatient Rehab Admission Criteria DBS Therapy • Patients may meet IRF admission criteria due to the change in clinical status: • Deep Brain Stimulation changes clinical status through symptom relief2 • Presence of ADL deficits is a patient selection criteria for DBS Therapy • Intensive rehabilitation contributes to the success of DBS therapy by improving ADL deficits 2 Rehncrona S;Johnels B;Widner H;Tornqvist AL;Hariz M;Sydow O. Long-term efficacy of thalamic deep brain stimulation for tremor: Double-blind assessments.Mov Disord 2003 Feb;18 (2): 163-70
American Academy of Neurology -PD Guidelines • DBS is included in the AAN PD Guidelines (released in April 2006) with the following key points: • “Ten to 20% of people with Parkinson disease may be eligible for surgical treatment.”1 • “Talk to your neurologist early in your disease to discuss the potential for future surgical treatment.”1 1AAN Guideline Summary for Patients and their Families: Medical and Surgical Treatment for Motor Fluctuations and Dyskinesia in Parkinson Disease, 2006
“ON” Time Without Dyskinesias Improves from 27% to 74% of a Patient’s Waking Day* 19% 27% 7% 49% 74%* 23% Before Surgery (n=96) 6 Months After SurgeryBilateral STN Activa® Implant (n=91) ‘ON’ with Dyskinesia ‘ON’ without Dyskinesia ‘OFF’ * The Deep-Brain Stimulation for Parkinson’s Disease Study Group. Deep-brain stimulation of the subthalamic nucleus for the pars interna of the globus pallidus in Parkinson’s disease. N Eng J Med. 2001;345:956-63.
Motor Symptoms Improvements Maintained After 5 Years • In a 5-year study, DBS significantly improved OFF-medication assessments of tremor, rigidity, and akinesia/bradykinesia *Results for STN
DBS efficacy for ET • 69% of Essential Tremor patients experience total or significant suppression of disabling tremor * • This results in significant reduction in disability • Stimulation-induced adverse effects include transient paresthesia, dysarthria, and disequilibrium • Many of the side effects were temporary or improved with adjustment of electrical parameters * Data on File. Medtronic, Inc.
“Conclusions: In this randomized controlled trial, deep brain stimulation was more effective than best medical therapy in alleviating disability in patients with moderate to severe PD with motor complications responsive to levodopa and no significant cognitive impairment.”