Download

1 / 6
60 likes | 82 Vues
Explore limited access to treatment due to high costs and lack of demand. Learn about Green Light Committee policy, treatment regimen costs, and global efforts to enhance access to quality care. Discover similarities between HIV and MDR-TB treatments and the importance of evidence-based policies.

E N D
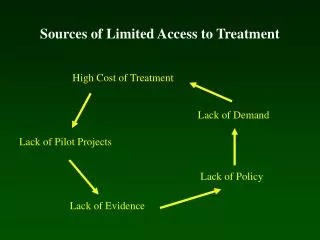
Sources of Limited Access to Treatment High Cost of Treatment Lack of Demand Lack of Pilot Projects Lack of Policy Lack of Evidence
Treatment Regimen Costs Standard Reference Country Cost (USA) High Income Country Average Cost Low Income Country Average Cost Green Light Committee Cost 60000 50000 40000 Per Patient Drug Cost (USD) 30000 20000 10000 0 HR HRES HRESZK Resistance Pattern Gupta, et al., Science 2001.
Linking Independent Concepts ACCESS RATIONAL USE GLC POLICY
Green Light Committee (GLC) • Releases preferentially-priced, quality-assured drugs • Decision process • application review • Instructions for Applying to the Green Light Committee for Access to Second-line Anti-TB Drugs • Guidelines for Establishing DOTS-Plus Pilot Projects for the Management of MDR-TB • site visit • Continual monitoring of projects • Technical assistance Gupta, et al. Trop Med Intl Health, 2001
Changing Global Health Policy • New guidelines for MDR-TB treatment • Expanding DOTS framework to include MDR-TB • HIV, public-private mix • Improving allocation of financial resources • Increasing new funds for TB control • Scaling up primary health care/capacity building • Bridging equity gap • No longer whether or not to treat patients, but how to best treat patients
Similarities between HIV and MDR-TB • Multidrug regimen given for extended periods with adverse events • Disproportionately affects disadvantaged • Access to drugs • Drug resistance • Laboratory requirements • Lack of standard international policy • Most experience in resource-wealthy settings