Download
1 / 71
710 likes | 715 Vues
Join the Utah Mental Health Counselors Association Conference in March 2019 to learn about a groundbreaking framework for achieving effective treatment outcomes. The presentation, led by Gray Otis, PhD, LCMHC, DCMHS-Trauma, will provide valuable insights and strategies for mental health counselors. Don't miss this opportunity to enhance your clinical practice and make a difference in the lives of your clients.

E N D
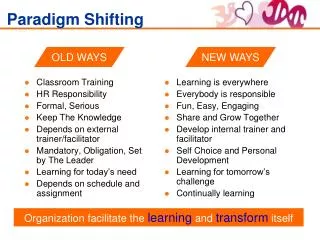
Shifting the ParadigmA Revolutionary Framework for Effective Treatment Outcomes • H. Gray Otis, PhD, LCMHC, DCMHS-Trauma • Utah Mental Health Counselors Association Conference – March, 2019
Gray Otis, PhD, LCMHC, CCMHC, DCMHS-T • AMHCA Diplomate, Clinical Mental Health Specialist in TraumaCurrent private practice – owner Vanguard Behavioral Health • Past clinical director of residential and intensive out patient treatment programsAMHCA Director of Program Coordination • AMHCA Liaison to AASCB and ACEs • 801-885-8585 • gray_otis@yahoo.com
Presentation Contributors • Gray Otis, PhD, LCMHC, CCMHC, DCMHS-T • AMHCA Diplomate, Clinical Mental Health Specialist in Trauma • He has been the clinical director of residential and intensive out patient treatment programs • Private practice – owner Vanguard Behavioral Health • Sandi Williams, MS, MA, LMFT • Specialist in trauma resolution and family counseling • She has co-facilitated a residential treatment program • Private practice – owner of the Meadows Counseling, adjunct professor at Utah Valley University • James Messina, PhD, Psychologist, CCMHC, DCMHS-T • AMHCA Diplomate, Clinical Mental Health Specialist in Trauma • He has served as a professor at Troy State University • Developed a library of on-line resources available at Coping.US
The AMHCA Initiatives AMHCA Disassociation from ACA
Clinical Mental Health Counselor Initiatives • CMHC Marketing Package – Video, Brochures, Bookmarks, etc. • Licensure Portability – Coalition with ACES, NBCC, AASCB • AMHCA Standards for the Practice of Clinical Mental Health Counseling • CMHC Declaration – Hippocratic Oath, a first in mental health • Credentialing Certifications: Clinical Specialist, Diplomate, Fellow • CMHC Professional Blueprint Career Model • Medicare Reimbursement
CMHC Marketing Package • Video – What is a Clinical Mental Health Counselor? • Printed marketing materials: • Information Brochures • Bookmarks • Handouts • Downloaded and available without cost
Clinical Mental Health Counselor Initiatives: • CMHC Marketing Package – Video, Information Brochures, Bookmarks, etc. • Licensure Portability – Coalition with ACES, NBCC, AASCB • AMHCA Standards for the Practice of Clinical Mental Health Counseling • CMHC Declaration – Hippocratic Oath, a first in mental health • Credentialing Certifications: Clinical Specialist, Diplomate, Fellow • CMHC Professional Blueprint Career Model • Medicare Reimbursement
Licensure portability • Coalition with ACES, NBCC, AASCB • Currently – drafted requirements • Intended to be compatible with state compacts • One size does not fit all states
Clinical Mental Health Counselor Initiatives: • CMHC Marketing Package – Video, Information Brochures, Bookmarks, etc. • Licensure Portability – Coalition with ACES, NBCC, AASCB • AMHCA Standards for the Practice of Clinical Mental Health Counseling • CMHC Declaration – Hippocratic Oath, a first in mental health • Credentialing Certifications: Clinical Specialist, Diplomate, Fellow • CMHC Professional Blueprint Career Model • Medicare Reimbursement
Standards for the Practice of Clinical Mental Health Counseling: • The Standards of Practice established in 1979 and updated ever since • Used by the Institute of Medicine to justify federal hiring and reimbursement • Includes: • Scope of Practice and Standards of Practice and Research • Clinical Practice Standards • Recommend AMHCA Training in the Knowledge and Skills: Biological Bases of Behavior Substance Use Disorders & Co-occurring Disorders Specialized Clinical Assessment Trauma Informed Care Technology Assisted Counseling (TAC) Integrated Behavioral Health Care Aging and Older Adults Standards and Competencies Child and Adolescent Standards and Competencies • New standards proposed for Military Counseling, Couples & Family, etc..
Clinical Mental Health Counselor Initiatives: • CMHC Marketing Package – Video, Information Brochures, Bookmarks, etc. • Licensure Portability – Coalition with ACES, NBCC, AASCB • AMHCA Standards for the Practice of Clinical Mental Health Counseling • CMHC Declaration – Hippocratic Oath, a first in mental health • Credentialing Certifications: Clinical Specialist, Diplomate, Fellow • CMHC Professional Blueprint Career Model • Medicare Reimbursement
Clinical Mental Health Counselor declaration • CMHC Declaration – the equivalent of an Hippocratic Oath • Recently approved by the Board of Directors • Voluntary • A public statement regarding professional ethics • Published in the latest AMHCA Advocate • May be downloaded without cost • Suitable for framing
Clinical Mental Health Counselor Initiatives: • CMHC Marketing Package – Video, Information Brochures, Bookmarks, etc. • Licensure Portability – Coalition with ACES, NBCC, AASCB • AMHCA Standards for the Practice of Clinical Mental Health Counseling • CMHC Declaration – Hippocratic Oath, a first in mental health • Credentialing Certifications: Clinical Specialist, Diplomate, Fellow • CMHC Professional Blueprint Career Model • Medicare Reimbursement
Credentialing Certifications: Specialist, Diplomate, Fellow Replaces the Diplomate & Clinical Mental Health Specialist (DCMHS) 1. Clinical Mental Health Counseling Specialist (CMHCS) in: Couples or Family Counseling Integrated Behavioral Health Care Counseling Substance Abuse and Co-occurring Disorders Developmental Disability Counseling Trauma Counseling Child and Adolescent Counseling Geriatric Counseling Military Counseling Each specialist credential requires training, supervision, & experience
Credentialing Certifications: Specialist, Diplomate, Fellow 2. Diplomate in Clinical Mental Health Practice (DCMHP): Earned by those who wish to be recognized Advanced Practice Establishes requirements and standards for counselors who have been fully licensed for at least 7 years and served the profession in positions of leadership, education, promotion of public mental health, etc.
Credentialing Certifications: Specialist, Diplomate, Fellow 3. Fellow in Clinical Mental Health Education and Research (FCMHER): Earned recognition in Advanced Education and Research Establishes requirements and standards for Counselor Educators who have been fully licensed for at least 7 years and served in education and research positions.
Clinical Mental Health Counselor Initiatives: • CMHC Marketing Package – Video, Information Brochures, Bookmarks, etc. • Licensure Portability – Coalition with ACES, NBCC, AASCB • AMHCA Standards for the Practice of Clinical Mental Health Counseling • CMHC Declaration – Hippocratic Oath, a first in mental health • Credentialing Certifications: Clinical Specialist, Diplomate, Fellow • CMHC Professional Blueprint Career Model • Medicare Reimbursement
Professional Blueprint Career Model • A career guide for counselors & a library of the profession’s pertinent documentation including: • History • Code of Ethics & CMHC Declaration • The Standards of Practice • Professional Development Guidance • Advanced Credentialing Certifications • Under current development with a publication date of this year
Clinical Mental Health Counselor Initiatives: • CMHC Marketing Package – Video, Information Brochures, Bookmarks, etc. • Licensure Portability – Coalition with ACES, NBCC, AASCB • AMHCA Standards for the Practice of Clinical Mental Health Counseling • CMHC Declaration – Hippocratic Oath, a first in mental health • Credentialing Certifications: Clinical Specialist, Diplomate, Fellow • CMHC Professional Blueprint Career Model • Medicare Reimbursement
Medicare Reimbursement: • Congressional bill for Medicare Reimbursement introduced again • Mental Health Access Improvement Act (S. 286) was re-introduced by Senator Barrasso (R-WY) and Senator Stabenow (D-MI) • Will allow counselors to bill Medicare for treating older adults with mental health conditions. • Both ACA and AMHCA support this legislative initiative • Still a concern regarding Congressional Budget Office accounting • Political winds are changing and Medicare Reimbursement will be enacted
Wrapping it up These are some of the current initiatives for our profession We have distinct advantages with respect to other mental health professions because of our focus on holistic health, strengths, and resilience The future looks very promising
Thank you for serving Questions?
Presentation Outline1) What Lies Beneath?2) Core Belief Development3) Shame vs Guilt4) HEART
Key Core Beliefs, Unlocking the HEART of Happiness & Health Available on Amazon Written for the public Includes workbook & online resources (KeyCoreBeliefs.org) Appendix for clinicians Can be used as an adjunct to therapy
Presentation Outline1) What Lies Beneath?2) Core Belief Development3) Shame vs Guilt4) HEART
Key Core Beliefs: What Lies Beneath • We propose that Negative Core Beliefs are schemas that lie at the genesis of nearly all mental health disorders. • Through the transformation of these injurious beliefs to Positive Core Beliefs, depression, anxiety, and trauma will be resolved with lasting results.
Powerfully held convictions about self: Consistent over time Can be either conscious or subconscious Based on prior experiences in childhood, adolescence, and adulthood Strongly linked to who we are – our unique sense of self Can often be expressed as “I am. . .” Statements (e.g. “I am a competitive person. . .I am competitive”) Key Core Beliefs Defined
Based on our experiences, we continually create self-beliefs – constructed reality of the self We accept our Key Core Beliefs as true – but – many are mistaken Each self-belief is either a Negative Core Belief or Positive Core Belief Negative Core Beliefs generally arise out of personally adverse interactions (“My friends don’t want to spend time with me. . .I am unattractive.”) Positive Core Beliefs arise out of personally affirmative interactions (“My teacher thinks I good at math. I must be pretty smart. . .I am smart.”) These self-beliefs filter our perceptions, thoughts, emotions, and actions. The accumulation of Key Core Beliefs develops our Self-Belief Identity Key Core Beliefs
How Key Core Beliefs act as filters Each event in our lives is influenced by our previous Key Core Beliefs and the emotions related to these deeply held convictions. As we perceive a new experience, our Key Core Beliefs immediately filter and influence our perceptions of the event. To illustrate:
Accumulating Key Core Beliefs Throughout the lifespan, both Positive and Negative Core Beliefs accumulate
Accumulating Key Core Beliefs Throughout the lifespan, both Positive and Negative Core Beliefs accumulate If Positive Core Beliefs predominate, the individualgenerally develops a constructive Self-Belief Identity Self-Belief Identity
Accumulating Key Core Beliefs Throughout the lifespan, both Positive and Negative Core Beliefs accumulate If Positive Core Beliefs predominate, the individualgenerally develops a constructive Self-Belief Identity However, if Negative Core Beliefs prevail, how would the individual be likely to perceive his or her Self-Belief Identity? Self-Belief Identity
Self-Belief Identity Our Self-Belief Identity creates either an antagonistic sense of self or a beneficial sense self: I am diabetic, I am sick – or – I have diabetes but I am tough and pretty healthy I am fat, I am ugly – or – I am healthy but I could lose some weight” Skilled therapists can help individuals develop added Positive Core Beliefs and a stronger, more constructive Self-Belief Identity Self-Belief Identity
Quiz: Negative to Positive Core Beliefs Negative Core BeliefsWhat would be a alternative Positive Core Belief? I am alone. I am hopeless. I am depressed. I am angry. I am critical. I am addicted. I am ashamed. I am lazy. I am unlovable.
Negative Core BeliefsWhat would be a alternative Positive Core Belief? I am alone. I am friendly. I am hopeless. I am hopeful. I am depressed. I am optimistic. I am angry. I am calm. I am critical. I am accepting. I am addicted. I am healthy. I am ashamed. I am okay. I am lazy. I am conscientious. I am unlovable. I am worthy to be loved. These are deeply held beliefs – not just positive affirmations Quiz: Negative to Positive Core Beliefs
Shame-Based Negative Core Beliefs Etiology Many Negative Core Beliefs originate from trauma or chronic distress • For example – use of the Adverse Childhood Experience questions: “Did a parent or other adult in the household often or very often… Swear at you, insult you, put you down, or humiliate you?” • Individuals suffer loss of attachment, low-grade anxiety, cultural conflicts, etc. • Deep seated emotions associated with shame may be manifested in any DSM disorder or medical condition (e.g. “I was often put down. . .I am worthless.”) • By attempting to numb severe negative emotions and shame, individuals simultaneously numb out joy and love • Often, there is a horrifying sense of isolation & helplessness
Distinguishing Between Guilt and Shame Guilt: “I did something wrong or terrible” Guilt motivates us to change Shame: “There is something wrong with me – I am terrible” Shame beliefs lead us to believe that we cannot change To resolve mental health disorders, mental health counselors must be skilled in helping individuals transform shame-based Negative Core Beliefs into Positive Core Beliefs
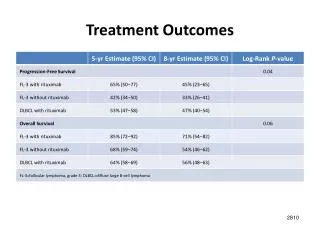
Mental health counselors need evidenced-based approaches to treat the underlying basis of co-occurring disorders Shame self-beliefs can be transformed into constructive, positive self- beliefs Outcome research shows that addressing underlying shame is highly effective in treating many DSM disorders including anxiety, PTSD, depression, addictions, and compulsive behaviors. All of these disorders have coupled, shame-based, Negative Core Beliefs If the beliefs are resolved, the symptoms resolve TheTransformation of Shame Self-Beliefs
Exercise: Shame-Based Beliefs Identify possible Shame Based, Negative Core Beliefs Teen-ager who was sexually abused in childhood
Exercise: Shame-Based Beliefs Identify possible Shame Based, Negative Core Beliefs Teen-ager who was sexually abused in childhood I am dirty, disgusting, undeserving, contemptible, etc.
Exercise: Shame-Based Beliefs Identify possible Shame Based, Negative Core Beliefs Teen-ager who was sexually abused in childhood I am dirty, disgusting, undeserving, contemptible, etc. Veteran whose close friend died in combat
Exercise: Shame-Based Beliefs Identify possible Shame Based, Negative Core Beliefs Teen-ager who was sexually abused in childhood I am dirty, disgusting, undeserving, contemptible, etc. Veteran whose close friend died in combat I am cowardly, deserve to die, disloyal, etc.
Exercise: Shame-Based Beliefs Identify possible Shame Based, Negative Core Beliefs Teen-ager who was sexually abused in childhood I am dirty, disgusting, undeserving, contemptible, etc. Veteran whose close friend died in combat I am cowardly, deserve to die, disloyal, etc. Woman who was emotionally devastated by divorce
Exercise: Shame-Based Beliefs Identify possible Shame Based, Negative Core Beliefs Teen-ager who was sexually abused in childhood I am dirty, disgusting, undeserving, contemptible, etc. Veteran whose close friend died in combat I am cowardly, deserve to die, disloyal, etc. Woman who was emotionally devastated by divorce I am unattractive, a failure, broken, etc.
Exercise: Shame-Based Beliefs Identify possible Shame Based, Negative Core Beliefs Teen-ager who was sexually abused in childhood I am dirty, disgusting, undeserving, contemptible, etc. Veteran whose close friend died in combat I am cowardly, deserve to die, disloyal, etc. Woman who was emotionally devastated by divorce I am unattractive, a failure, broken, etc. An adult who was extensively criticized as a child
Exercise: Shame-Based Beliefs Identify possible Shame Based, Negative Core Beliefs Teen-ager who was sexually abused in childhood I am dirty, disgusting, undeserving, contemptible, etc. Veteran whose close friend died in combat I am cowardly, deserve to die, disloyal, etc. Woman who was emotionally devastated by divorce I am unattractive, a failure, broken, etc. An adult who was extensively criticized as a child I am stupid, a mess, disappointing, etc.