Download
1 / 56
630 likes | 1.12k Vues
Chapter 6 Laboratory Diagnostics in Thrombosis and Hemostasis. Peng Liming. OVERVIEW OF HEMOSTASIS. Primary and Secondary Hemastasis

E N D
Chapter 6 Laboratory Diagnostics inThrombosis and Hemostasis Peng Liming
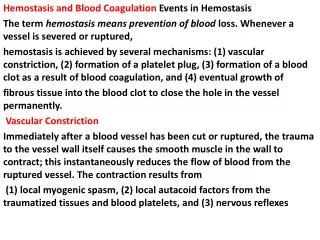
OVERVIEW OF HEMOSTASIS • Primary and Secondary Hemastasis Hemostasis may be defined as the process that maintains flowing blood in a fluid state and prevents loss of blood from sites of vascular disruption. This definition implies two major components: The first, a potent procoagulant mechanism that is capable of forming stable hemostatic plugs at sites of vascular disruption; and second, regulatory systems that confine normal hemostatic plug formation to sites of vascular disruption.
Key structural features of normal resting platelets are depicted(Figure 6-1.)
The formation of a hemostatic plug usually begins when the vessel wall is damaged, exposing the thrombogenic bendothelial tissue to blood(Figure 6-5. )
Regulation of Hemostasis There are multiple systems that work in a synergistic manner to regulate the extent of clot formation. They include intact endothelium, platelet (Table 6-3), fibrin clot formation (Table 6-4), and the relative important regulatory systems are platelet, fibrin clot formation which is consisted of tissue factor pathway inhibitor (TFPI), serine protease inhibitors (serpins), protein C system and the fibrinolytic system(Table 6-5, Fig 6-6).
Fibrinolytic mechanism and degradation products(Figure 6-6. )
LABORATORY METHODS FOR EVALUATION OF PLATELET FUNCTION A variety of laboratory techniques may be used to assess platelet function, but a limited number of techniques are necessary for most clinical situations (Table 6-6)
Laboratory techniques for evaluation of platelet function(1)(TABLEe 6-6. )
Laboratory techniques for evaluation of platelet function(2)(TABLE 6-6. )
The Bleeding Time The bleeding time (BT) is a commonly performed test to assess global function of primary hemostasis. A number of techniques for determining the bleeding time have been described, but the most commonly performed method is the template bleeding time(TBT) using a disposable device.
Analysis of von Willebrand Factor Commonly used procedures to evaluate vWF include vWF antigen concentration (vWF:ag), ristocetin cofactor activity(vWF:Rcof), vWF binding to collagen or recombinant glycoprotein lb (GP Ib), the platelet aggregation response to ristocetin, and vWF multimeric analysis. Immunoelectrophoresis was once the only practical method available for determination of vWF:ag, but enzyme-linked immunosorbant assays (ELISAs) and automated immunoassays are now available.
Platelet Response To Agonists Platelet aggregation studies are used to assess the response of platelets to a variety of agonists. Platelet aggregation is most commonly performed by a turbidimetric method using platelet-rich plasma but also can be performed by an impedance method that utilizes either whole blood or platelet-rich plasma (PRP).
Nomnal (C) and abnormal (Pt) aggregation responses for ADP, collagen, epinephrine, and ristocetin (Figure 6-7.)
Flow cytometry has emerged as a powerful tool for the analysis of platelet function. Platelet activation is associated with surface expression of proteins not found on quiescent platelets. Analysis of these proteins has been used to evaluate in vivo platelet activation, which occurs in a variety of clinical settings.
Flow diagram for diagnosis of abnormalities of platelet function (Figure 6-8. ).
LABORATORY EVALUATION OF HEMOSTATIC DISORDERS There are a number of reasons why the hemostatic system may be evaluated during the clinical management of patients. Common reasons include therapeutic drug monitoring, presurgical evaluation of hemostasis, evaluation of a possible bleeding tendency, evaluation of a possible thrombotic tendency, evaluation for the possibility of a circulating lupus anticoagulant, evaluation for the possibility of disseminated intravascular coagulation, and evaluation for other specific disorders.
Routine presurgical evaluation of hemostasis remains a controversial topic. In general, routine preoperative bleeding times, prothrombin times (PTs) and activated partial thromboplastin times (APTTs) do not accurately predict the risk of bleeding during surgery. Laboratory evaluation of hemostasis is indicated whenever the clinical and/or medical history suggests the possibility of altered hemostasis. As hemostasis is a balanced system with potent procoagulant and regulatory mechanisms, bleeding or thrombotic disorders can arise whenever this balance is disturbed.
Evaluation of a Potential Bleeding Disorder The clinical history of a patient with a potential bleeding disorder is used to determine whether the patient truly does have a bleeding problem, whether the problem is likely to be congenital or acquired, and whether the defect is related to altered primary hemostasis, secondary hemostasis, or regulation of hemostasis.
Following the clinical history, routine screening tests are commonly performed. These include the platelet count and bleeding time to assess platelet function and the PT and APTT to assess fibrin clot formation. Note that these screening tests do not assess fibrin stabilization or fibrinolysis.
The PT evaluates the extrinsic system of coagulation, beginning with activation of coagulation by tissue factor/VIIa, and is sensitive to defects in fibrinogen, prothrombin, factor V, factor X,and factor VII. APTT evaluates the intrinsic system of coagulation and is sensitive to defects in fibrinogen, prothrombin, factor V, factor X, factor VIII, factor IX, factor XI, factor XII, prekallikrein, and HMW kininogen.
Common patterns associated with bleeding disorders Based on the results of the clinical history and screening laboratory tests, a limited number of patterns emerge (Table 6-8).
Laboratory Analysis of Coagulation The PT and APTT provide an arbitrary dissection of coagulation into the intrinsic (APTT) system and the extrinsic (PT) system. Although in reality this division is artificial, it is very useful from the standpoint of patient evaluation.
Diagnosis of inherited coagulation factor deficiencies(Figure 6-9.)
The thrombin time (TT) is a very useful test and it is often overlooked. TT may be abnormal in a variety of clinical situations. TT is extremely useful in ruling out the presence of heparin in a patient sample. The finding of a prolonged TT that corrects with the addition of protamine is virtually diagnostic of heparin.
Evaluation of A Potential Thrombotic Tendency As with the evaluation of bleeding disorders, the evaluation of a potential thrombotic tendency begins with a thorough medical history. One of the primary goals of the history is to determine the likelihood of a congenital defect. There are no screening assays that assess the overall function of the regulatory system of coagulation or the degree of activation of the procoagulant systems. Therefore, the laboratory approach to potential thrombotic disorders involves measuring selected individual components of the regulatory systems.
Evaluation of D-dimer in the diagnosis of suspected DVT & PE (Figure 6-10.)
COAGULATION ABMORIVALITIES Hereditary Disorders Of Coagulation Proteins Hemophilia A (Factor VIII Deficiency) Hemophilia A is an X-linked inherited disorder of factor VIII (Antihemophiliac Globulin). The incidence is approximately 1:5,000 males. As previously discussed, factor VIII is a critical cofactor in the intrinsic coagulation pathway at the level of factor X activation.
The laboratory diagnosis of hemophilia A is relatively straightforward. In the majority of cases, APTT will be prolonged while PT and BT will be within normal limits. Factor VIIIC assays are necessary to establish the diagnosis. Patients with severe hemophilia A will have factor VIIIC levels, which are less than 1% (0.01 U/ml).
Hemophilia B (Factor IX Deficiency) Hemophilia B is also a sex-linked disorder. Christinas disease and factor IX deficiency are frequently used synonyms. The incidence of hemophilia B is approximately 1:40,000 to 1:50,000 population. However, in certain groups such as the Amish and East Indians, hemophilia B occurs as often as hemophilia A. Varying degrees of hemophilia B have been recognized with severe <l% (0.01U/ml), moderate <5% (0.01 to 0.05 U/ml) and mild >5% (>0.05 U/ml) phenotypes analogous to factor VIII deficiency.
Hemophilia C (Factor XI Deficiency) Factor XI deficiency is an incompletely autosomal-recessivehereditary disorder. The majority of factor XI deficiency occursin individuals of Jewish descent. In an extensive study by Seligsohn of Ashkenazi Jews, the frequency of homozygotes for factorXI deficiency was 0.1% to 0.3% whereas the heterozygotes werefound in 5.5% to 11.0%.
Afibrinogenemia And Hypofibrinogenemia Afibrinogenemia is a rare disorder inherited in an autosomal-recessive pattern. There often is a variable history of clinical bleeding. Laboratory abnormalities of all of the standard screening tests are present. No end point is detected with the PT, APTT, or thrombin time. The bleeding time may be slightly prolonged and platelet aggregation studies typically show a lack of response to the usual agonists (ADP, epinephrine, and collagen).
Hypofibrinogenemic patients are characterized by a fibrinogen level, which is less than 100 mg/dl. Often these patients have a mild bleeding tendency with an autosomal dominant or, in some cases, an autosomal-recessive pattern of inheritance. In many cases, hypofibrinogenemic patients will have normal PT and APTT results. However, typically the thrombin time will be abnormal. Clottable and immunologic fibrinogen assay results are decreased thus establishing the diagnosis.
Dysfibrinogenemia Hereditary dysfibrinogenemia is inherited in an autosornal-dominant pattern. These abnormal fibrinogen molecules are caused by mutations, which result in single arnino-acid alteration in one of the three fibrinogen chains (a-alpha, b-beta, or gamma chains). Laboratory findings include normal or only minimally prolonged values for PT and APTT. Typically, the thrombin time is prolonged as is the reptilase time. The abnormal thrombin time usually cannot be corrected by the addition of proramine or calcium. Laboratory diagnosis relies on the demonstration of a discrepancy between the level of clottable fibrinogen and antigenic fibrinogen.
Acquired DisordersOf Coagulation Proteins Oral Anticoagulant Therapy Oral anticoagulant therapy is based on administration of coumarin or its derivatives. This class of drugs blocks the reductase enzyme in the vitamin K pathway resulting in increased levels of nonfunctional vitamin K epoxide.
The monitoring of oral anticoagulant therapy has relied upon the PT and variants of the PT(INR). For many years there has been an international controversy regarding the optimal test system tomonitor oral anticoagulants. In order to report an INR value, it is necessary to know the International Sensitivity Index (ISI) for the thromboplastin being used as well as the geometric mean of the PT range.
The introduction of the INR has emphasized the need for lower doses of oral anticoagulants. In the past when PT results were reported as ratios, the therapeutic range was typically quoted as PT ratios of 1.5 to 2.5. With the use of the INR, it is now evident the majority of patients are satisfactorily anticoagulated with INRs of 2.0 to 3.0. As a consequence, it is anticipated the incidence of bleeding in patients receiving oral anticoagulant therapy will significantly decrease.
Disseminated Intravascular Coagulation (DIC) DIC may be encountered in a variety of different clinical situations. Clinical examples would include amnionic fluid embolus, head injuries, neurosurgery, and certain malignancies. Some tumor cells appear to have a specific enzyme (cysteine protease), which will directly activate factor X. Alternatively with endothelial injury, there may be activation of the extrinsic pathway leading to DIC.