
Correlation of Hand-Foot Skin Reaction with Treatment Efficacy in Advanced Pancreatic Cancer
This study assesses the correlation between hand-foot skin reaction (HFS) and treatment efficacy in patients with advanced pancreatic cancer treated with gemcitabine/capecitabine and erlotinib. Using data from the AIO-PK0104 clinical trial, we found that patients experiencing HFS showed a significantly prolonged time to treatment failure (TTF2) and overall survival (OS) compared to those without HFS. The findings support the potential predictive value of HFS for treatment outcomes, particularly following capecitabine treatment.

Correlation of Hand-Foot Skin Reaction with Treatment Efficacy in Advanced Pancreatic Cancer
E N D
Presentation Transcript
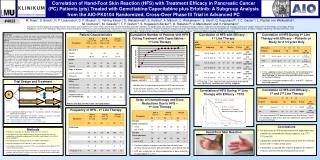
Correlation of Hand-Foot Skin Reaction (HFS) with Treatment Efficacy in Pancreatic Cancer (PC) Patients (pts) Treated with Gemcitabine/Capecitabine plus Erlotinib: A Subgroup Analysis from the AIO-PK0104 Randomized, Cross-Over Phase III Trial in Advanced PC #4023 M. Haas1, S. Boeck1, R. P. Laubender2, D. P. Modest1, U. Vehling-Kaiser3, D. Waldschmidt4, E. Kettner5, A. Märten6, C. Winkelmann7, S. Klein8, G. Kojouharoff9, T. C. Gauler10, L. Fischer von Weikersthal11, M. Clemens12, M. Geissler13, T. F. Greten14, S. Hegewisch-Becker15, O. Rubanov16, U. Mansmann2 and V. Heinemann1 1Department of Hematology and Oncology, Klinikum Grosshadern and Comprehensive Cancer Center, LMU Munich; 2Institute for Medical Informatics, Biometry and Epidemiology, LMU Munich;3Practice for Medical Oncology, Landshut; 4Department of Hematology and Oncology, University of Cologne; 5Department of Hematology and Oncology, Klinikum Magdeburg; 6University of Heidelberg; 7Department of Internal Medicine, Krankenhaus Lutherstadt-Wittenberg; 8Department of Internal Medicine IV, Klinikum Bayreuth; 9Practice for Medical Oncology, Darmstadt; 10West German Tumor Center, University Hospital Essen; 11Gesundheitszentrum St. Marien, Amberg; 12Mutterhaus der Boromaeerinnen, Trier; 13Department of Gastroenterology and Oncology, Klinikum Esslingen; 14Medical School Hannover; 15Private Practice for Oncology, Hamburg; 16Practice for Medical Oncology, Hameln; all in Germany Patient Characteristics Cumulative Number of Patients with HFS During Treatment with Capecitabine – 1st Line Therapy Correlation of HFS with Efficacy – 1st Line Therapy Correlation of HFS During 1st Line Therapy with Efficacy – Patients on Study for ≥ 3 Cycles Only Background: AIO-PK 0104 investigated the efficacy and safety of gemcitabine/erlotinib (G/E) followed by capecitabine (C) vs. C/E followed by G. The present subgroup analysis evaluated the correlation between C-associated skin toxicity and outcome parameters in PC. Methods: Within this multicenter phase III trial, pts with confirmed advanced PC were randomly assigned to 1st-line treatment with either C (2,000 mg/m2/d, d1-14 q d21) plus E (150 mg/d, arm A) or G (1,000 mg/m2 over 30 min weekly x 7, then d1, 8, 15 q d28) plus E (150 mg/d, arm B). A cross-over to either G (arm A) or C (arm B) was performed after treatment failure (e. g. disease progression or unacceptable toxicity). Time to treatment failure after 1st- and 2nd-line therapy (TTF2) was the primary study endpoint. Treatment-related skin toxicity was evaluated separately for each treatment arm/each regimen based on NCI-CTCv2. Results: Of 279 eligible pts, 47 had locally advanced, 232 had metastatic disease and 141 pts received second-line chemotherapy. For the present subgroup analysis data on skin toxicity were available from 255 pts. For the 73 pts (29%) with a HFS (any grade documented at any time during the treatment strategy), TTF2 and OS both were significantly prolonged compared to pts without HFS (7.4 vs 4.0 months, p<0.001 and 9.7 vs 5.5 months, p=0.002, respectively). Considering HFS during 1st-line treatment in 123 pts within the CE arm, these results could be confirmed for the 47 pts (38%) with a documented HFS of any grade (TTF2: 7.6 vs. 3.2 months, p<0.001; OS: 10.2 vs. 4.4 months, p=0.001). In pts receiving 1st-line treatment with G/E (n=132) no difference in outcome was observed for pts with (n=13) or without (n=119) HFS of any grade (TTF2: 5.7 vs. 4.2 months, p=0.375; OS: 8.4 vs. 6.6 months, p=0.505). Conclusions: The current subgroup analysis of AIO-PK0104 supports the assumption of a correlation between HFS in PC pts treated with capecitabine or capecitabine/erlotinib and efficacy endpoints like TTF2 and OS. A capecitabine-associated HFS thus might be predictive for efficacy in patients with advanced PC. Overall: 47 pts. with HFS • In this subgroup analysis, only patients still on protocol after completion of 3 cycles (time of first tumour assessment) were included (i.e. patients who were defined as assessable for treatment efficacy) • Differences in outcome between HFS + and HFS – patients remained apparent Trial Design and Treatment • HFS during 1st line treatment with capecitabine and erlotinib was significantly correlated with efficacy endpoints • Median time to capecitabine-attributed HFS was two cycles • In 36 out of 47 patients (77%) HFS was documented for the first time within the first three treatment cycles Arm A Correlation of HFS with Efficacy – 1st and 2nd Line Therapy 2nd line: gemcitabine 1st line: capecitabine + erlotinib Correlation of HFS During 1st Line Therapy with Efficacy - TTF2 R 1:1 TTF 1 Arm B Delay of Chemotherapy and Dose Reductions Due to HFS – 1st Line Therapy Arm A: capecitabine + erlotinib → gemcitabine N=281 1st line: gemcitabine + erlotinib 2nd line: capecitabine Patients with data on HFS (n=255, safety population) No HFS: 3.2 months HFS grades 1-3: 7.6 months HR 0.46 (95%CI 0.32-0.67), p<0.001 Frequency of HFS - 1st Line Therapy TTF 2 Arm A: capecitabine 2.000 mg/m2/d p.o. d1-14, q d21 plus erlotinib, 150 mg/d p.o.; followed by gemcitabine Arm B: gemcitabine 1.000 mg/m2 over 30 min i.v. weekly x 7, then d1, 8, 15 q d28 plus erlotinib, 150 mg/d p.o.; followed by capecitabine TTF 1: time-to-treatment failure after 1st line therapy TTF 2: time-to-treatment failure after 1st and 2nd line therapy • The occurrence of HFS documented at any time during 1st or 2nd line therapy (in both arms) also was significantly correlated with treatment efficacy Conclusions Methods • The occurrence of HFS during treatment with capecitabine plus erlotinib was correlated with efficacy endpoints (e. g. TTF1, TTF2 and OS) • Capecitabine-attributed HFS occurred early within the treatment course (after a median of two cycles) • Capecitabine-associated HFS might be predictive for treatment efficacy in patients with advanced pancreatic cancer Hand-Foot Skin Reaction • Definition of hand-foot-skin reaction (HFS): NCI-CTC version 2 • Retrospective, post-hoc subgroup analysis based on toxicity data from the prospective, multicenter randomized AIO-PK0104 study (Boeck S et al, ASCO 2010: LBA#4011) • Safety population including 255 of the 274 eligible study patients • Separate subgroups for HFS during 1st and 2nd line therapy • Correlation of HFS with the primary (TTF2) and secondary study endpoints (TTF1, OS) for treatment efficacy • Analyses were repeated for patients who were on study for at least 3 cycles and therefore had at least one tumour assessment (i.e. patients who were defined as assessable for treatment efficacy) • Treatment delays and dose reductions overall were more common during treatment with gemcitabine and erlotinib (arm B) • HFS was responsible for delayed application or dose reductions of capecitabine in < 10%





















