Download
1 / 59
590 likes | 805 Vues
Eosinophilic Penumonia. Wael Batobara. History. 80 y Male X smoker 50y 15pp Childhood Bronchial Astma Non resolving SOB , Cough , Wheeze 3/52 Orthopnea But no PND. History. Low grade fever , minimal sputum No chest pain or leg pain No hematuria , joint swelling or pain

E N D
Eosinophilic Penumonia Wael Batobara
History • 80 y Male X smoker 50y 15pp • Childhood Bronchial Astma • Non resolving SOB , Cough , Wheeze 3/52 • Orthopnea But no PND
History • Low grade fever , minimal sputum • No chest pain or leg pain • No hematuria , joint swelling or pain • No runny nose ,post nasal drip, heart burn
History • No change in environment • No contact with sick person , No pets • Increased use of bronchodilator without response • Seen at Selkerik treated with Abx without responsetransferred to HSC Dec 17th
History • PMH : Childhood Asthma Infrequent attacks No Intubations or ICU admissions HTN ,DM with proteinuria Osteoprosis & Chronic Xerosis No IHD , CHF
History • PSH : TURP • Rx : Adavir , Terbutaline , Metformine ,Ramipril , Alendronate , Vit D , Ca & ECASA
Examination • Temp 37.8 RR18 Sat 90-95 on 2-5 lit. O2 • BP 130/70 HR 90 • ENT : no erythema ,post nasal drip • Chest : resonant ,Good BS bilateral Wheeze , minimal crackles
Examination • CVS : JVP N S1+S2+0 • Abd & LL N • No skin rash , arthritis • CNS NAD
Investigations • CBC WBC 14.4 Eosinophil 44% Hb 120 MCV N & Plt N • Coagulation N • BUN , Creat & lytes N • Cardiac enzymes & EKG N
Investigations • UA –ve casts • ABG on 3lit. O2 PaO2 70 PCO2 30 PH 7.47 HCO3 23 • CXR & CT
Hospital Course • Seen by Chest Med working Dx Eosinophilic pneumonia Churg Strauss Syn • Open lung Bx was arranged • Started on Systemic steroids , Nebulizers
Hospital Course • Septic work up –ve • Improvement on steroids 1-2 lit. O2 94% • Open lung Bx & BAL on Dec 20th Chronic Eosinophilic Pneumonia • ANCA both P & C –ve
Hospital Course • WBC 14-16 Neut 85% Initially for 2 days • Gradual worsening SOB & hypoxemia Dec23-25th • Simultaneous recurrence of eosinophilia WBC 18 Eosinophil 80% • Progressive hypoxemia ICU Dec26th
Hospital Course • Mechanical Ventilation • Echo poor window • Swan No evidence of Lt HF • Bronchoscopy Dec 31st -ve
Hospital Course • Persistent eosinophilia • Cyclophospamide 5 days • Extubated but didn’t do well High FIO2 • Didn’t want reintubation • Trial BiPAP
Hospital Course • EET CS stenotrophomonas Treated with Cipro & Ceftaz • Septra was added empirically • Kept worsening with decreased LOC • Still on BiPAP
Hospital Course • A fib Amiodarine • WBC 23 Eosinophils 65% • Family meeting Direction of care Palliative • Patient died Jan 9th
Chronic Eosinophilic Pneumonia • Causes of Pulmonary eosinophilia • Chronic eosinophilic pneumonia CEP Presentation , Dx , Rx , prognosis • Association between CEP & asthma • Acute Eosinophilic Pneumonia
Pulmonary Eosinophilia • Lung infiltrates with peripheral , BAL or tissue eosinophilia • Heterogenous group of diseases • Infections Helmenthic Vs Non Helminthic Helminthic infections different presentations depending of duration of contact with lung parynchema & host immune response
Helminthic Infections • Loffler’s Syndrome Transpulmonary passage of migrating larvae Ascaris , Hookworm & Strongyloides Parasitemia larvae penetrate alveoli & ascends the airways to reach GI Dry irritating cough & substernal pain Fever, SOB & Wheeze +/- hemoptysis Migratory infiltrates with eosinophilia
Helminthic Infections • Direct parynchemal invasion Associated with initial eosinophilia Echinococcosis,Cysticercosis &Pargonimos • Visceral larva migrans invasion of lung parynchema which is not essential in the life cycle of the worm • Tropical Eosinophilia immune response to blood & lymphatic stages of the worm Wuchereria bancrofti & Brugia malayi
Pulmonary Eosinophilia • Non helminthic infection : TB & Cocci • Drug reaction NSAID Abx (penicillin , Nitrofu, Penatmidine) Phenytoin , Ranitidien , GM GCSF • Toxins Inhaled heroin , cocaine or scotchguard rubber & sulfite Dust & smokes
Pulmonary Eosinophilia • ABPA asthma , central bronchiectasis • Malignancy 1ry lung or 2ry • Idiopathic Hypereosinophilic syndrome tissue infilitration without obvious cause • Churg Straus Syndrome • Acute eosinophilic Pneumonia • Chronic eosinophilic pneumonia
Chronic Eosinophilic Pneumonia • First described by Carrington 1969 9 females with background of asthma & other atopic diseases Worsening SOB ,bilateral lung infiltrates Eeosinophilia peripheral or BAL Dramatic reponse to steroid with recurrence after tapering steroids
Chronic Eosinophilic Pneumonia • Retrospective study 62 patients • GERM”O”P registery French collaborative group Rare(Orphan)Pulmonary disease 700 Pt 1997 Medicine (Baltimore) Sept98
Chronic Eosinophilic Pneumonia • Inclusion 1) Predominantly Peripheral infiltrates 2) Blood eosinophilia >or= 1 g/l or eosin >40% of BAL 3) Symptoms >2 weekslung Open lung Bx was not required
Chronic Eosinophilic Pneumonia • 77 patients initially • 15 excluded: 3 didn’t meet inclusion 2 exposure to drugs 4 insufficient data 3 +ve serology to helminthes , Asperg. 3 other Dx malignancy ,sarcoidosis Churg Strauss Synd
Chronic Eosinophilic Pneumonia • 42 females & 20 males Mean age 45y • 6.5% smokers • 63% atopic asthma, rhinitis, conjuctivitis dermatitis or drug reaction • Preceding Asthma duration 10 years
Chronic Eosinophilic Pneumonia • Mean time from symptoms & Dx 20-65 W • No patient required mechanical ventilation • Hemoptysis was not major symptom • 9.7% extrapulmonary involvement arthritis ,skin rash , pericarditis & hepatitis
Chronic Eosinophilic Pneumonia • CXR : Bilateral 75.8% Upper lobes 46.8% Vs Lower lobes 11.3% Upper & Lower 41.9% Migratory opacities 25.5% Small pleural effusion 6.5% Bilateral hilar LN 1 case.
Chronic Eosinophilic Pneumonia • CT was available for 40 pt Ground glass & dense infiltrates 72.5% 1Pt small effusion 2Pt with LN 1 hilar & 1 mediastinal
Chronic Eosinophilic Pneumonia • 95% Pt eosinophilia >1 g/l Mean 5.5 • 5%Pt eosinophilia < 1 with 40% BAL • 4.4% ANA +ve • 1 patient +ve PANCA no evidence of other organ involvement
Chronic Eosinophilic Pneumonia • PFT: was available in 50 pt 36% obstructive Vs 32% restrictive ?element of airway disease In 20% pt without prior Dx of asthma Obstructive pattern was found • ABG : was available in 44 pt 65% hypoxemia <10 Kpa
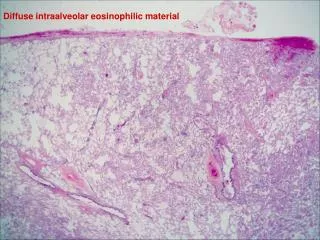
Chronic Eosinophilic Pneumonia • Open Lung bx 6.5% open lung Bx All open Bx interstitial infiltrate & alveolar exudate of eosinophils 2 open Bx additional finding of BOOP
Chronic Eosinophilic Pneumonia • Transbronchial Bx 12.5 % transbronchial Bx 5/8 transbronch Bx interstitial & alveolar infiltrates with eosinophilis 2/5 no abnormality 1/5 organizing pneumonia (Bx was 2 after systemic steroid)
Chronic Eosinophilic Pneumonia • Bronchial Bx : eosinophilic infiltrate in 3 pt Non had prior Asthma One developed asthma later • LN Bxhyperplasia & esniophilic infiltrate • Liver Bx regenerative hepatitis with eosin.
Chronic Eosinophilic Pneumonia • Treatment : All except one received systemic steroids Mean dose 1 mg/kg Rapid clinical improvement 48 hours 82% including extrapulmonary involvement Radiological improvement 70% within week Variable steroid tapering
Chronic Eosinophilic Pneumonia • Relapse 48 patients had relapse 12/48 recurrent 28/48 after being off steroid for 55week ? Rapid taper may be harmless 20/48 while on tapering dose 10 mg/day Realapse at different radiological locations Relapse responded well to steroid
Chronic Eosinophilic Pneumonia • Follow up 46 pt had follow up >1 y Mean follow up 6y 16 pt had asthma 4/16 were diagnosed after CEP Dx 9 pt fixed obstructive PFT both groups were maitained on systemic steroid 4 died non respiratory related
CEP & BA • Retrospective study • Same registry GERM”O”P 1435 pt 2002 • Will presence of BA at CEP Dx will affect presentation or outcome ? • Assess severity & evolution of BA since CEP Dx Euro Resp Jr 2003 Vol 22
CEP & BA • 53 pt 34 females & 19 male Mean age 43 • 27 BA +ve prior & 26 BA -ve • 34 BA+ve atVs 7 BA+ve after CEP Vs BA -ve • 42 Pt follow up>1y 25 BA +ve & 17 BA-ve
CEP & BA • Higher IgE in asthmatics • Tendency to lower BAL eosin. in asthmatics • Tendency to lower eosin. in Inhaledsteroid gp
CEP & BA • 26/53 BA prior to CEP Dx 76-92 months • 9 pt mild Vs 12 pt moderate Vs 4 pt severe • 60% asthmatics required systemic steroid for an exacerbation
CEP & BA • 42/53 pt Long term follow up • Mean FU 87+/-62 months • At last FU 65% Pt on inhaled steroid for BA & 56% on systemic steroid for excacerbation
CEP & BA • Asthmatics & inhaled steroid had lower rate of relapse ? Inhaled steroids effect • Asthma severity increased after CEP Dx ? Equal F:M ratio & higher smoker in non asthmatics • No significant difference in relapse between pt maintained on or weaned off systemic steroid at last FU